The coronary arteries wrap around the entire heart and both lungs . The two main branches are the left coronary artery and right coronary artery.
The arteries can additionally be categorized based on the area of the
heart for which they provide circulation. These categories are called epicardial (above the epicardium, or the outermost tissue of the heart) and microvascular (close to the endocardium, or the innermost tissue of the heart).
Reduced function of the coronary arteries can lead to decreased
flow of oxygen and nutrients to the heart. Not only does this affect
supply to the heart muscle itself, but it also can affect the ability of
the heart to pump blood throughout the body. Therefore, any disorder or
disease of the coronary arteries can have a serious impact on health,
possibly leading to angina, a heart attack, and even death.
Structure
The
coronary arteries are mainly composed of the left and right coronary
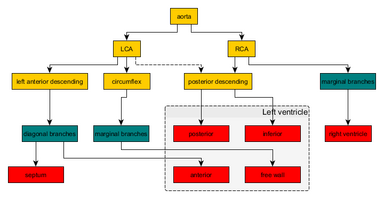
arteries, both of which give off several branches, as shown in the
'coronary artery flow' figure.
The left coronary artery arises from the aorta within the left cusp of the aortic valve and feeds blood to the left side of the heart. It branches into two arteries, the left anterior descending and the left circumflex. The left anterior descending artery perfuses the interventricular septum and anterior wall of the left ventricle.
The left circumflex artery perfuses the left ventricular free wall. In
approximately 33% of individuals, the left coronary artery gives rise to
the posterior descending artery
which perfuses the posterior and inferior walls of the left ventricle.
Sometimes a third branch is formed at the fork between left anterior
descending and left circumflex arteries, known as a ramus or intermediate artery.
The right coronary artery (RCA) originates within the right cusp of the aortic valve. It travels down the right coronary sulcus, towards the crux of the heart. The RCA primarily branches into the right marginal arteries, and, in 67% of individuals, gives place to the posterior descending artery.
The right marginal arteries perfuse the right ventricle and the
posterior descending artery perfuses the left ventricular posterior and
inferior walls.
There is also the conus artery, which is only present in
about 45 percent of the human population, and which provides collateral
blood flow to the heart when the left anterior descending artery is
occluded.
Narrowing of the arteries can be caused by a process known as atherosclerosis (most common), arteriosclerosis, or arteriolosclerosis. This occurs when plaques (made up of deposits of cholesterol and other substances) build up over time in the walls of the arteries. Coronary artery disease (CAD) or ischemic heart disease are the terms used to describe narrowing of the coronary arteries.
As the disease progresses, plaque buildup can partially block blood flow to the heart muscle. Without enough blood supply (ischemia), the heart is unable to work properly, especially under increased stress. Stable angina is chest pain on exertion that improves with rest. Unstable angina
is chest pain that can occur at rest, feels more severe, and/or last
longer than stable angina. It is caused by more severe narrowing of the
arteries.
Heart attack
A heart attack results from a sudden plaque rupture and formation of a thrombus (blood clot) that completely blocks blood flow to a portion of the heart, leading to tissue death (infarct).
CAD can also result in heart failure or arrhythmias.
Heart failure is caused by chronic oxygen deprivation due to reduced
blood flow, which weakens the heart over time. Arrhythmias are caused by
inadequate blood supply to the heart that interferes with the heart's
electric impulse.
The coronary arteries can constrict as a response to various stimuli, mostly chemical. This is known as a coronary reflex.
There is also a rare condition known as spontaneous coronary artery dissection, in which the wall of one of the coronary arteries tears, causing severe pain.
Unlike CAD, spontaneous coronary artery dissection is not due to plaque
buildup in arteries, and tends to occur in younger individuals,
including women who have recently given birth or men who do intense
exercise.
Coronary artery dominance is described as the coronary artery
that give branches to supply the right posterior descending artery and
supplies the inferior wall of the heart. In 80 to 85% of the population,
the right coronary artery supplies the posterior descending artery,
making it right heart dominant while in 7 to 13% of the population, the
left coronary artery supplies the posterior descending artery, making it
left heart dominant. In 7 to 8% of the population, both right and left
coronary arteries supplies the posterior descending artery, making it
right and left co-dominance. Narrowing of coronary arteries is more
frequent in those who are left dominant when compared to those who have
right dominant or co-dominant hearts.
The word corona is a Latin word meaning "crown", from the Ancient Greekκορώνη (korōnè, "garland, wreath"). It was applied to the coronary arteries because of a notional resemblance (compare the photos).
The word arterie in Anglo-French (artaire in Old French, and artērium
in Latin) means "windpipe" and "an artery". It was applied to the
coronary arteries because the arteries do not contain blood after death.
A sensorium (/sɛnˈsɔːrɪəm/) (pl.: sensoria) is the apparatus of an organism's perception considered as a whole. It is the "seat of sensation"
where it experiences, perceives and interprets the environments within
which it lives. The term originally entered English from the Late Latin
in the mid-17th century, from the stem sens- ("sense"). In earlier use it referred, in a broader sense, to the brain as the mind's organ (Oxford English Dictionary
1989). In medical, psychological, and physiological discourse it has
come to refer to the total character of the unique and changing sensory
environments perceived by individuals. These include the sensation,
perception, and interpretation of information about the world around us
by using faculties of the mind such as senses, phenomenal and psychological perception, cognition, and intelligence.
McLuhan, like his mentor Harold Innis, believed that media were biased according to time and space. He paid particular attention to what he called the sensorium, or the effects of media on our senses, positing that media affect us by manipulating the ratio of our senses. For example, the alphabet
stresses the sense of sight, which in turn causes us to think in
linear, objective terms. The medium of the alphabet thus has the effect
of reshaping the way in which we, collectively and individually,
perceive and understand our environment in what has been termed the Alphabet Effect.
Focusing on variations in the sensorium across social contexts,
these theorists collectively suggest that the world is explained and
experienced differently depending on the specific "ratios of sense" that
members of a culture
share in the sensoria they learn to inhabit (Howes 1991, p. 8). More
recent work has demonstrated that individuals may include in their
unique sensoria perceptual proclivities that exceed their cultural
norms; even when, as in the history of smell in the West, the sense in
question is suppressed or mostly ignored (Classen, Howes and Synnott
1994).
This interplay of various ways of conceiving the world could be compared to the experience of synesthesia,
where stimulus of one sense causes a perception by another, seemingly
unrelated sense, as in musicians who can taste the intervals between
notes they hear (Beeli et al., 2005), or artists who can smell
colors. Many individuals who have one or more senses restricted or lost
develop a sensorium with a ratio of sense which favors those they
possess more fully. Frequently the blind or deaf speak of a compensating
effect, whereby their sense of touch or smell becomes more acute,
changing the way they perceive and reason about the world; especially
telling examples are found in the cases of "wild children", whose early
childhoods were spent in abusive, neglected, or non-human environments,
both intensifying and minimizing perceptual abilities (Classen 1991).
Development of unique sensoria in cultures and individuals
Although some consider these modalities abnormal, it is more likely that these
examples demonstrate the contextual and socially learned nature of
sensation. A 'normal' sensorium and a 'synesthetic' one differ based on the
division, connection, and interplay of the body's manifold sensory
apparatus. A synesthete has simply developed a different set of
relationships, including cognitive or interpretive skills which deliver
unique abilities and understanding of the world (Beeli et al., 2005).
The sensorium is a creation of the physical, biological, social, and cultural environments of the individual organism and its relationships while being in the world.
What is considered a strange blurring of sensation from one perspective, is a normal and 'natural'
way of perception of the world in another, and indeed many individuals
and their cultures develop sensoria fundamentally different from the
vision-centric modality of most Western science and culture. One
revealing contrast is the thought of a former Russian on the matter:
The dictionary of the Russian language...defines the sense of
touch as follows: "In reality all five senses can be reduced to
one---the sense of touch. The tongue and palate sense the food; the ear,
sound waves; the nose, emanations; the eyes, rays of light." That is
why in all textbooks the sense of touch is always mentioned first. It
means to ascertain, to perceive, by body, hand or fingers (Anonymous
1953).
As David Howes explains:
The reference to Russian textbooks treating touch first, in
contrast to American psychology textbooks which always begin with sight,
is confirmed by other observers (Simon 1957) and serves to highlight
how the hierarchization of the senses can vary significantly even
between cultures belonging to the same general tradition (here, that of
"the West") (2003, pp. 12-13).
Sensory ecology and anthropology
These sorts of insights were the impetus for the development of the burgeoning field of sensory anthropology,
which seeks to understand other cultures from within their own unique
sensoria. Anthropologists such as Paul Stoller (1989) and Michael Jackson (1983, 1989) have focused on a critique of the hegemony
of vision and textuality in the social sciences. They argue for an
understanding and analysis that is embodied, one sensitive to the unique
context of sensation of those one wishes to understand. They believe
that a thorough awareness and adoption of other sensoria is a key
requirement if ethnography is to approach true understanding.
A related area of study is sensory (or perceptual) ecology.
This field aims at understanding the unique sensory and interpretive
systems all organisms develop, based on the specific ecological
environments they live in, experience and adapt to. A key researcher in
this field has been psychologist James J. Gibson,
who has written numerous seminal volumes considering the senses in
terms of holistic, self-contained perceptual systems. These exhibit
their own mindful, interpretive behaviour, rather than acting simply as
conduits delivering information for cognitive processing, as in more representational philosophies of perception or theories of psychology (1966, 1979). Perceptual systems detect affordances
in objects in the world, directing attention towards information about
an object in terms of the possible uses it affords an organism.
The individual sensory systems of the body are only parts of these broader perceptual ecologies, which include the physical apparatus of sensation, the environment
being sensed, as well as both learned and innate systems for directing
attention and interpreting the results. These systems represent and
enact the information (as an influence which leads to a transformation)
required to perceive, identify or reason about the world, and are
distributed across the very design and structures of the body, in
relation to the physical environment, as well as in the concepts and
interpretations of the mind. This information varies according to
species, physical environment, and the context of information in the
social and cultural systems of perception, which also change over time
and space, and as an individual learns through living. Any single
perceptual modality may include or overlap multiple sensory structures,
as well as other modes of perception, and the sum of their relations and
the ratio of mixture and importance comprise a sensorium. The
perception, understanding, and reasoning of an organism is dependent on
the particular experience of the world delivered by changing ratios of
sense.
Clouded sensorium
A clouded sensorium, also known as an altered sensorium, is a medical condition characterized by the inability to think clearly or concentrate. It is usually synonymous with, or substantially overlapping with, altered level of consciousness.
It is associated with a huge variety of underlying causes from drug
induced states to pathogenic states induced by disease or mineral
deficiency to neurotrauma.
Reality tunnel is a theory that, with a subconscious set of mental filters formed from beliefs and experiences, every individual interprets the same world differently, hence "Truth is in the eye of the beholder". It is similar to the idea of representative realism, and was coined by Timothy Leary (1920–1996). It was further expanded on by Robert Anton Wilson (1932-2007), who wrote about the idea extensively in his 1983 book Prometheus Rising.
Wilson and Leary co-wrote a chapter in Leary's 1988 book Neuropolitique (a revised edition of the 1977 book Neuropolitics), in which they explained further:
The gene-pool politics which monitor power struggles
among terrestrial humanity are transcended in this info-world, i.e. seen
as static, artificial charades. One is neither coercively manipulated
into another's territorial reality nor forced to struggle against it
with reciprocal game-playing (the usual soap opera dramatics). One
simply elects, consciously, whether or not to share the other's reality
tunnel.
Considerations
Every
kind of ignorance in the world all results from not realizing that our
perceptions are gambles. We believe what we see and then we believe our
interpretation of it, we don't even know we are making an interpretation
most of the time. We think this is reality. – Robert Anton Wilson
The idea does not necessarily imply that there is no objective truth; rather that our access to it is mediated through our senses, experience, conditioning,
prior beliefs, and other non-objective factors. The implied individual
world each person occupies is said to be their reality tunnel. The term
can also apply to groups of people united by beliefs: we can speak of
the fundamentalist Christian reality tunnel or the ontological naturalist reality tunnel.
A parallel can be seen in the psychological concept of confirmation bias—the
human tendency to notice and assign significance to observations that
confirm existing beliefs, while filtering out or rationalizing away
observations that do not fit with prior beliefs and expectations. This
helps to explain why reality tunnels are usually transparent to their
inhabitants. While it seems most people take their beliefs to correspond
to the "one true objective reality", Robert Anton Wilson emphasizes
that each person's reality tunnel is their own artistic creation,
whether they realize it or not.
Wilson — like John C. Lilly in his 1968 book Programming and Metaprogramming in the Human Biocomputer
— relates that through various techniques one can break down old
reality tunnels and impose new reality tunnels by removing old filters
and replacing them with new ones, with new perspectives on reality—at
will. This is attempted through various processes of deprogramming using
neuro-linguistic programming, cybernetics, hypnosis, biofeedback devices, meditation, controlled use of hallucinogens,
and forcibly acting out other reality tunnels. Thus, it is believed
one's reality tunnel can be widened to take full advantage of human
potential and experience reality on more positive levels. Robert Anton
Wilson's Prometheus Rising is (among other things) a guidebook to the exploration of various reality tunnels.
Similar ideas
In line with Kantian thought, as well as the work of Norwood Russell Hanson, studies have indeed shown
that our brains "filter" the data coming from our senses. This
"filtering" is largely unconscious and may be influenced—more-or-less in
many ways, in societies and in individuals—by biology, cultural constructs including education and language (such as memes), life experiences, preferences and mental state,belief systems (e.g. world view, the stock market), momentary needs, pathology, etc.
An everyday example of such filtering is our ability to follow a
conversation, or read, without being distracted by surrounding
conversations, once called the cocktail party effect.
In his 1986 book Waking Up, Charles Tart—an Americanpsychologist and parapsychologist
known for his psychological work on the nature of
consciousness—introduced the phrase "consensus trance" to the lexicon.
Tart likened normal waking consciousness to hypnotic trance. He
discussed how each of us is from birth inducted to the trance of the
society around us. Tart noted both similarities and differences between hypnotic trance induction and consensus trance induction. (See G. I. Gurdjieff).
Some disciplines—Zen for example, and monastic schools such as Sufism—seek to overcome such conditioned realities by returning to less thoughtful and channeled states of mind. Similarly, the philosophy of lifePyrrhonism seeks to overcome these conditioned realities by inducing epoche (suspension of judgment) through skeptical arguments.
Constructivism is a modern psychological response to reality-tunneling.
For Wilson, a fully functioning human ought to be aware
of their reality tunnel, and be able to keep it flexible enough to
accommodate, and to some degree empathize with, different reality
tunnels, different "game rules", different cultures.... Constructivist
thinking is the exercise of metacognition to become aware of our reality
tunnels or labyrinths and the elements that "program" them.
Constructivist thinking should, ideally, decrease the chance that we
will confuse our map of the world with the actual world.... [This
philosophy] is currently expressed in many Eastern
consciousness-exploration techniques.
Neuropsychiatry is a branch of medicine that deals with psychiatry as it relates to neurology, in an effort to understand and attribute behavior to the interaction of neurobiology and social psychology factors. Within neuropsychiatry, the mind is considered "as an emergent property of the brain", whereas other behavioral and neurological specialties might consider the two as separate entities. Those disciplines are typically practiced separately.
Currently, neuropsychiatry has become a growing subspecialty of psychiatry as it closely relates the fields of neuropsychology and behavioral neurology,
and attempts to utilize this understanding to better treat illnesses
that fall under both neurological and mental disorder classifications
(e.g., autism, ADHD, Tourette's syndrome).
The case for the rapprochement of neurology and psychiatry
Given
the considerable overlap between these subspecialities, there has been a
resurgence of interest and debate relating to neuropsychiatry in
academia over the last decade.
Most of this work argues for a rapprochement of neurology and
psychiatry, forming a specialty above and beyond a subspecialty of
psychiatry. For example, Professor Joseph B. Martin, former Dean of Harvard Medical School and a neurologist
by training, has summarized the argument for reunion: "the separation
of the two categories is arbitrary, often influenced by beliefs rather
than proven scientific observations. And the fact that the brain and
mind are one makes the separation artificial anyway." These points and some of the other major arguments are detailed below.
Mind/brain monism
Neurologists have focused objectively on organic nervous system pathology, especially of the brain, whereas psychiatrists have laid claim to illnesses of the mind. This antipodal
distinction between brain and mind as two different entities has
characterized many of the differences between the two specialties.
However, it has been argued that this division is fictional; evidence
from the last century of research has shown that our mental life has its
roots in the brain.
Brain and mind have been argued not to be discrete entities but just
different ways of looking at the same system (Marr, 1982). It has been
argued that embracing this mind/brain monism
may be useful for several reasons. First, rejecting dualism implies
that all mentation is biological, which provides a common research
framework in which understanding and treatment of mental disorders can
be advanced. Second, it mitigates widespread confusion about the
legitimacy of mental illness by suggesting that all disorders should
have a footprint in the brain.
In sum, a reason for the division between psychiatry and neurology
was the distinction between mind or first-person experience and the
brain. That this difference is taken to be artificial by proponents of
mind/brain monism supports a merge between these specialties.
Causal pluralism
One of the reasons for the divide is that neurology traditionally looks at the causes of disorders from an "inside-the-skin" perspective (neuropathology, genetics) whereas psychiatry looks at "outside-the-skin" causation (personal, interpersonal, cultural).
This dichotomy is argued not to be instructive and authors have argued
that it is better conceptualized as two ends of a causal continuum. The benefits of this position are: firstly, understanding of etiology will be enriched, in particular between brain and environment. One example is eating disorders,
which have been found to have some neuropathology (Uher and Treasure,
2005) but also show increased incidence in rural Fijian school girls
after exposure to television (Becker, 2004). Another example is schizophrenia, the risk for which may be considerably reduced in a healthy family environment (Tienari et al., 2004).
It is also argued that this augmented understanding of etiology
will lead to better remediation and rehabilitation strategies through an
understanding of the different levels in the causal process where one
can intervene. It may be that non-organic interventions, like cognitive behavioral therapy (CBT), better attenuate disorders alone or in conjunction with drugs. Linden's (2006) demonstration of how psychotherapy has neurobiological commonalities with pharmacotherapy
is a pertinent example of this and is encouraging from a patient
perspective as the potentiality for pernicious side effects is decreased
while self-efficacy is increased.
In sum, the argument is that an understanding of the mental
disorders must not only have a specific knowledge of brain constituents
and genetics (inside-the-skin) but also the context (outside-the-skin)
in which these parts operate (Koch and Laurent, 1999). Only by joining
neurology and psychiatry, it is argued, can this nexus be used to reduce
human suffering.
Organic basis
To further sketch psychiatry's history shows a departure from structural neuropathology, relying more upon ideology (Sabshin, 1990). A good example of this is Tourette syndrome, which Ferenczi (1921), although never having seen a patient with Tourette syndrome, suggested was the symbolic expression of masturbation
caused by sexual repression. However, starting with the efficacy of
neuroleptic drugs in attenuating symptoms (Shapiro, Shapiro and Wayne,
1973) the syndrome has gained pathophysiological support (e.g. Singer,
1997) and is hypothesized to have a genetic basis too, based on its high
inheritability (Robertson, 2000). This trend can be seen for many
hitherto traditionally psychiatric disorders (see table) and is argued
to support reuniting neurology and psychiatry because both are dealing with disorders of the same system.
Linking traditional psychiatric symptoms or disorders to brain structures and genetic abnormalities. (This table is in not exhaustive but provides some neurological bases to psychiatric symptoms.)
Atypical serotonin system, right frontal and temporal lobe dysfunction, changes to mesolimbic dopamine pathways
Kaye et al. (2005), Uher and Treasure (2005), Olsen (2011), Slochower (1987)
Improved patient care
Further, it is argued that this nexus will allow a more refined nosology of mental illness to emerge thus helping to improve remediation and rehabilitation
strategies beyond current ones that lump together ranges of symptoms.
However, it cuts both ways: traditionally neurological disorders, like Parkinson's disease, are being recognized for their high incidence of traditionally psychiatric symptoms, like psychosis and depression (Lerner and Whitehouse, 2002). These symptoms, which are largely ignored in neurology,
can be addressed by neuropsychiatry and lead to improved patient care.
In sum, it is argued that patients from both traditional psychiatry and
neurology departments will see their care improved following a reuniting
of the specialties.
Better management model
Schiffer et al. (2004) argue that there are good management and financial reasons for rapprochement.
US institutions
"Behavioral
Neurology & Neuropsychiatry" fellowships are accredited by the
United Council for Neurologic Subspecialties (UCNS; www.ucns.org), in a manner analogous to the accreditation of psychiatry and neurology residencies in the United States by the American Board of Psychiatry and Neurology (ABPN).
The American Neuropsychiatric Association
(ANPA) was established in 1988 and is the American medical subspecialty
society for neuropsychiatrists. ANPA holds an annual meeting and offers
other forums for education and professional networking amongst
subspecialists in behavioral neurology and neuropsychiatry as well as
clinicians, scientists, and educators in related fields. American
Psychiatric Publishing, Inc. publishes the peer-reviewed Journal of Neuropsychiatry and Clinical Neurosciences, which is the official journal of ANPA.
International organizations
The International Neuropsychiatric Association was established in 1996.
INA holds congresses biennially in countries around the world and
partners with regional neuropsychiatric associations around the world to
support regional neuropsychiatric conferences and to facilitate the
development of neuropsychiatry in the countries/regions where those
conferences are held. Prof. Robert Haim Belmaker is the current President of the organization whereas Prof. Ennapadam S Krishnamoorthy serves as President-Elect with Dr. Gilberto Brofman as Secretary-Treasurer.
The British NeuroPsychiatry Association (BNPA) was founded in 1987
and is the leading academic and professional body for medical
practitioners and professionals allied to medicine in the UK working at
the interface of the clinical and cognitive neurosciences and
psychiatry.
In 2011, a non-profit professional society named Neuropsychiatric Forum
(NPF) was founded. NPF aims to support effective communication and
interdisciplinary collaboration, develop education schemes and research
projects, organize neuropsychiatric conferences and seminars.
Patients in such a dramatically altered state of consciousness
present unique problems for diagnosis, prognosis and treatment.
Assessment of cognitive functions remaining after a traumatic brain
injury is difficult. Voluntary movements may be very small, inconsistent
and easily exhausted. Quantification of brain activity differentiates
patients who sometimes only differ by a brief and small movement of a
finger.
Consciousness is a complex and multifaceted concept, divided into two main components: Arousal and Awareness.
Arousal is associated with functional brainstem neuron populations projecting to both thalamic and cortical neurons.
Therefore, the assessment of reflexes (Using the Glasgow Coma Scale) is
important to investigate the functional integrity of the brainstem.
Awareness is thought to be related with functional integrity of the
cerebral cortex and its subcortical connections. The most important
point regarding the classification of disorders of consciousness is,
that consciousness cannot be measured objectively by any machine,
although many scoring systems have been developed for the quantification
of consciousness and neuroimaging techniques are important tools for
clinical research, extending our understanding of underlying mechanisms
involved.
Disorders in consciousness represent immense social and ethical issues
because the diagnosis is methodologically complex and needs careful
interpretation. Also the ethical framework must be further developed to
guide research in these patients.
In locked-in syndrome the patient has awareness, sleep-wake cycles, and meaningful behavior (viz., eye-movement), but is isolated due to quadriplegia and pseudobulbar palsy,
resulting from the disruption of corticospinal and corticobulbar
pathways. Locked-in syndrome is a condition in which a patient is aware
and awake but cannot move or communicate verbally due to complete
paralysis of nearly all voluntary muscles in the body except for the
eyes. Eye or eyelid movements are the main method of communication. Total locked-in syndrome is a version of locked-in syndrome where the eyes are paralyzed as well.
In a minimally conscious state,
the patient has intermittent periods of awareness and wakefulness. The
criteria for minimally conscious state, that patients are not in a vegetative state
but are not able to communicate consistently. This means, that patients
have to show limited but reproducible signs of awareness of themself or
their environment. This could be following of simple commands,
intelligible speech or purposeful behavior (including movements or
affective behavior in relation to external stimuli, but not reflexive
activity).
Further improvement towards full conscious recovery is more likely in
this state than in the vegetative state, but still some patients remain
in the MCS constantly.
In a persistent vegetative state,
the patient has sleep-wake cycles, but lacks awareness, is not able to
communicate and only displays reflexive and non-purposeful behavior. The
term refers to an organic body that is able to grow and develop devoid
of intellectual activity or social intercourse.
The diagnosis of the vegetative state should be questioned when there
is any degree of sustained and reproducible visual pursuit or fixation
or response to threatening gestures.
This state reflects an intact brainstem and allied structures but
severely damaged white and gray matter in both cerebral hemispheres. The
preservation of these structures maintains arousal and automatic
functions.
The overall metabolism drops in average to 40-50% of the normal range.
After four weeks in a vegetative state (VS), the patient is classified
as in a persistent vegetative state. Here the metabolism drops to 30-40%
of the normal range but seems to be a result of trans-synaptic neuronal
degeneration.
Although the diagnosis is problematic, the formal absence of any sign of
conscious perception or deliberate action is essential.
This diagnosis can be further classified as a permanent vegetative state
(PVS) after approximately 1 year of being in a vegetative state after
traumatic brain injury
Like coma, chronic coma
results mostly from cortical or white-matter damage after neuronal or
axonal injury, or from focal brainstem lesions. Usually the metabolism
in the grey matter decreases to 50-70% of the normal range. The patient
lacks awareness and arousal. The patient lies with eyes closed and is
not aware of self or surroundings. Stimulation cannot produce
spontaneous periods of wakefulness and eye-opening, unlike patients in
vegetative state. In medicine, a coma (from the Greek κῶμα koma, meaning
deep sleep) is a state of unconsciousness, lasting more than six hours
in which a person cannot be awakened, fails to respond normally to
painful stimuli, light, sound, lacks a normal sleep-wake cycle and does
not initiate voluntary actions. Although, according to the Glasgow Coma Scale,
a person with confusion is considered to be in the mildest coma. But
cerebral metabolism has been shown to correlate poorly with the level of
consciousness in patients with mild to severe injury within the first
month after traumatic brain injury (TBI).
A person in a state of coma is described as comatose. In general
patients surviving a coma recover gradually within 2–4 weeks. But
recovery to full awareness and arousal is not always possible. Some
patients do not progress further than vegetative state or minimally
conscious state and sometimes this also results in prolonged stages
before further recovery to complete consciousness.
Although a coma patient may appear to be awake, they are unable
to consciously feel, speak, hear, or move. For a patient to maintain
consciousness, two important neurological components must function
impeccably. The first is the cerebral cortex which is the gray matter
covering the outer layer of the brain. The other is a structure located
in the brainstem, called reticular activating system (RAS or ARAS). Injury to either or both of these components is sufficient to cause a patient to experience a coma.
Brain death is the irreversible end of all brain activity, and
function (including involuntary activity necessary to sustain life). The
main cause is total necrosis of the cerebral neurons following loss of
brain oxygenation. After brain death
the patient lacks any sense of awareness; sleep-wake cycles or
behavior, and typically look as if they are dead or are in a deep
sleep-state or coma. Although visually similar to a comatose state such
as persistent vegetative state, the two should not be confused. Criteria
for brain death differ from country to country. However, the clinical
assessments are the same and require the loss of all brainstem reflexes
and the demonstration of continuing apnea in a persistently comatose patient (< 4 weeks).
Functional imaging using PET or CT scans, typically show a hollow skull
phenomenon. This confirms the absence of neuronal function in the whole
brain.
Patients classified as brain dead are legally dead and can qualify as
organ donors, in which their organs are surgically removed and prepared
for a particular recipient.
Brain death is one of the deciding factors when pronouncing a
trauma patient as dead. Determining function and presence of necrosis
after trauma to the whole brain or brain-stem may be used to determine
brain death, and is used in many states in the US.
Methodological problems
Metabolic
studies are useful, but they are not able to identify neural activity
within a specific region to specific cognitive processes. Functionality
can only be identified at the most general level: Metabolism in cortical
and subcortical regions that may contribute to cognitive processes.
At present, there is no established relation between cerebral metabolic rates of glucose or oxygen as measured by PET
and patient outcome. The decrease of cerebral metabolism occurs also
when patients are treated with anesthetics to the point of
unresponsiveness. Lowest value (28% of normal range) have been reported
during propofol anesthesia. Also, deep sleep represents a phase of
decreased metabolism (down to 40% of the normal range)
In general, quantitative PET studies and the assessment of cerebral metabolic rates depends on many assumptions.
PET, for example, requires a correction factor, the lumped constant,
which is stable in healthy brains. There are reports that a global
decrease of this constant emerges after a traumatic brain injury.
But, not only the correction factors change due to TBI.
Another issue is the possibility of anaerobic glycolysis that could
occur after TBI. In such a case, the glucose levels measured by the PET
are not tightly connected to the oxygen consumption of the patient's
brain.
Third point regarding PET scans is the overall measurement per unit
volume of brain tissue. The imaging can be affected by the inclusion of
metabolically inactive spaces e.g. cerebrospinal fluid in the case of gross hydrocephalus, which artificially lowers the calculated metabolism.
Also, the issue of radiation exposure must be considered in patients
with already severely damaged brains and preclude longitudinal or
follow-up studies.
Ethical issues
Disorders of consciousness present a variety of ethical concerns.
Most obvious is the lack of consent in any treatment decisions. Patients
in PVS or MCS are not able to decide for the possibility of withdrawal
of life-support. It is also a general question whether they should
receive life-sustaining therapy and, if so, for what duration. The
problems regarding a patient's consent also account for neuroimaging
studies. Without patient's consent, such studies are perceived as
unethical. Additionally, only few patients have created advance directives before losing decision-making capacity.
Typically, approval must be obtained from family or legal
representatives depending on governmental and hospital guidelines but,
even with the consent of representatives, researchers have been refused
grants, ethics committee approval and publication.
Social issues arise from the enormous costs associated with
people who have disorders of consciousness, especially chronic comatose
and vegetative patients, when recovery is highly unlikely and treatment
in the ICU is considered futile by clinicians.
In addition to the aforementioned problems, the question rises why
medical resources were being used not for the broader public good but
for patients who seemed to have only little to gain from them.
Nevertheless, the irreversibility of these conditions remains an open
question. Some studies demonstrated that some patients with disorders of
consciousness may be aware despite clinical unresponsiveness. These findings could have a major impact on ethical and social issues.
An altered level of consciousness is any measure of arousal other than normal. Level of consciousness (LOC) is a measurement of a person's arousability and responsiveness to stimuli from the environment. A mildly depressed level of consciousness or alertness may be classed as lethargy; someone in this state can be aroused with little difficulty. People who are obtunded have a more depressed level of consciousness and cannot be fully aroused. Those who are not able to be aroused from a sleep-like state are said to be stuporous. Coma is the inability to make any purposeful response. Scales such as the Glasgow coma scale have been designed to measure the level of consciousness.
An altered level of consciousness can result from a variety of
factors, including alterations in the chemical environment of the brain
(e.g. exposure to poisons or intoxicants), insufficient oxygen or blood flow in the brain, and excessive pressure within the skull. Prolonged unconsciousness is understood to be a sign of a medical emergency. A deficit in the level of consciousness suggests that both of the cerebral hemispheres or the reticular activating system have been injured. A decreased level of consciousness correlates to increased morbidity (sickness) and mortality (death).
Thus it is a valuable measure of a patient's medical and neurological
status. In fact, some sources consider level of consciousness to be one
of the vital signs.
Definition
Scales
and terms to classify the levels of consciousness differ, but in
general, reduction in response to stimuli indicates an altered level of
consciousness:
People who possess the ability to monitor and control their own
cognitive processes in addition to meeting all the criteria indicative
of a normal level of consciousness. In the field of cognitive neuroscience, metacognitive monitoring and control have been viewed as functions of the prefrontal cortex,
which receives sensory input signals from divergent cortical regions
and implements control through feedback loops which are established
utilizing the underlying mechanisms of neuroplasticity (see chapters by Schwartz & Bacon and Shimamura, in Dunlosky & Bjork, 2008).
Assessment of LOC involves checking orientation:
people who are able promptly and spontaneously to state their name,
location, and the date or time are said to be oriented to self, place,
and time, or "oriented X3". A normal sleep stage from which a person is easily awakened is also considered a normal level of consciousness. "Clouding of consciousness" is a term for a mild alteration of consciousness with alterations in attention and wakefulness.
People who do not respond quickly with information about their name, location, and the time are considered "obtuse" or "confused". A confused person may be bewildered, disoriented, and have difficulty following instructions.
The person may have slow thinking and possible memory time loss. This
could be caused by sleep deprivation, malnutrition, allergies,
environmental pollution, drugs (prescription and nonprescription), and
infection.
The most commonly used tool for measuring LOC objectively is the Glasgow Coma Scale (GCS). It has come into almost universal use for assessing people with brain injury,
or an altered level of consciousness. Verbal, motor, and eye-opening
responses to stimuli are measured, scored, and added into a final score
on a scale of 3–15, with a lower score being a more decreased level of
consciousness.
Others
The AVPU scale is another means of measuring LOC: people are assessed to determine whether they are alert, responsive to verbal stimuli, responsive to painful stimuli, or unresponsive. To determine responsiveness to voice, a caregiver speaks to, or, failing that, yells at the person.
Responsiveness to pain is determined with a mild painful stimulus such
as a pinch; moaning or withdrawal from the stimulus is considered a
response to pain. The ACDU scale, like AVPU, is easier to use than the GCS and produces similarly accurate results. Using ACDU, a patient is assessed for alertness, confusion, drowsiness, and unresponsiveness.
Although the neural science behind alertness, wakefulness, and arousal are not fully known, the reticular formation is known to play a role in these. The ascending reticular activating system is a postulated group of neural connections that receives sensory input and projects to the cerebral cortex through the midbrain and thalamus from the reticular formation.
Since this system is thought to modulate wakefulness and sleep,
interference with it, such as injury, illness, or metabolic
disturbances, could alter the level of consciousness.
Normally, stupor and coma are produced by interference with the brain stem, such as can be caused by a lesion or indirect effects, such as brain herniation. Mass lesions in the brain stem normally cause coma due to their effects on the reticular formation. Mass lesions that occur above the tentorium cerebelli normally do not significantly alter the level of consciousness unless they are very large or affect both cerebral hemispheres.
Diagnosis
Assessing LOC involves determining an individual's response to external stimuli. Speed and accuracy of responses to questions and reactions to stimuli such as touch and pain are noted. Reflexes, such as the cough and gag reflexes, are also means of judging LOC. Once the level of consciousness is determined, clinicians seek clues for the cause of any alteration.
Usually the first tests in the ER are pulse oximetry to determine if
there is hypoxia, serum glucose levels to rule out hypoglycemia. A urine
drug screen may be sent. A CT head is very important to obtain to rule
out bleed. In cases where meningitis is suspected, a lumbar puncture
must be performed. A serum TSH is an important test to order. In select
groups consider vitamin B12 levels. Checking serum ammonia is
particularly advised in neonatal coma to discern inborn errors of metabolism.
Treatment
depends on the degree of decrease in consciousness and its underlying
cause. Initial treatment often involves the administration of dextrose if the blood sugar is low as well as the administration of oxygen, naloxone and thiamine.
The USDA's original food pyramid, from 1992 to 2005
A food pyramid is a representation of the optimal number of servings to be eaten each day from each of the basic food groups. The first pyramid was published in Sweden in 1974.The 1992 pyramid introduced by the United States Department of Agriculture (USDA) was called the "Food Guide Pyramid" or "Eating Right Pyramid". It was updated in 2005 to "MyPyramid", and then it was replaced by "MyPlate" in 2011.
Amid high food prices in 1972, Sweden's National Board of Health and Welfare
developed the idea of "basic foods" that were both cheap and
nutritious, and "supplemental foods" that added nutrition missing from
the basic foods. Anna-Britt Agnsäter, chief of the test kitchen for Kooperativa Förbundet
(a cooperative Swedish retail chain), held a lecture the next year on
how to illustrate these food groups. Attendee Fjalar Clemes suggested a
triangle displaying basic foods at the base. Agnsäter developed the idea
into the first food pyramid, which was introduced to the public in 1974
in KF's Vi magazine. The pyramid was divided into basic foods at the base, including milk, cheese, margarine, bread, cereals and potato; a large section of supplemental vegetables and fruit; and an apex of supplemental meat, fish and egg.
The pyramid competed with the National Board's "dietary circle", which
KF saw as problematic for resembling a cake divided into seven slices,
and for not indicating how much of each food should be eaten. While the
Board distanced itself from the pyramid, KF continued to promote it.
Food pyramids were developed in other Scandinavian countries, as well as West Germany, Japan and Sri Lanka. The United States later developed its first food pyramid in 1992.
Food pyramid published by the WHO and FAO
The World Health Organization,
in conjunction with the Food and Agriculture Organization, published
guidelines that can be effectively represented in a food pyramid
relating to objectives in order to prevent obesity, improper nutrition,
chronic diseases and dental caries based on meta-analysis though they represent it as a table rather than as a "pyramid". The
structure is similar in some respects to the USDA food pyramid, but
there are clear distinctions between types of fats, and a more dramatic
distinction where carbohydrates are categorized on the basis of free sugars
versus sugars in their natural form. Some food substances are singled
out due to the impact on the target issues that the "pyramid" is meant
to address. In a later revision, however, some recommendations are
omitted as they automatically follow other recommendations while other
sub-categories are added. The reports quoted here explain that where
there is no stated lower limit in the table below, there is no requirement for that nutrient in the diet.
A "simplified" representation of the "Food Pyramid" from the 2002 Joint WHO/FAO Expert Consultation recommendations
≥ 30 g/day (as part of the 400 g of fruit and vegetables)
Total dietary fiber
27–40 g/day
From foods
Non-starch polysaccharide (NSP)
16–24 g/day
From foods
All percentages are percentages of calories,
not of weight or volume. To understand why, consider the determination
of an amount of "10% free sugar" to include in a day's worth of
calories. For the same amount of calories, free sugars take up less
volume and weight, being refined and extracted from the competing carbohydrates in their natural form. In a similar manner, all the items are in competition for various categories of calories.
The representation as a pyramid is not precise, and involves
variations due to the alternative percentages of different elements, but
the main sections can be represented.
The USDA's food pyramid from 2005 to 2011, MyPyramid
The USDA food pyramid was created in 1992 and divided into six
horizontal sections containing depictions of foods from each section's
food group. It was updated in 2005 with black and white vertical wedges
replacing the horizontal sections and renamed MyPyramid. MyPyramid was often displayed with the food images absent, creating a more abstract design.
In an effort to restructure food nutrition guidelines, the USDA rolled out its new MyPlate
program in June 2011. My Plate is divided into four slightly different
sized quadrants, with fruits and vegetables taking up half the space,
and grains and protein making up the other half. The vegetables and
grains portions are the largest of the four.
A modified food pyramid was proposed in 1999 for adults aged over 70.
Vegetables
A vegetable
is a part of a plant consumed by humans that is generally savory but is
not sweet. A vegetable is not considered a grain, fruit, nut, spice, or herb. For example, the stem, root, flower, etc., may be eaten as vegetables. Vegetables contain many vitamins and minerals;
however, different vegetables contain different balances of
micronutrients, so it is important to eat a wide variety of types. For
example, orange and dark green vegetables typically contain vitamin A, dark green vegetables contain vitamin C, and vegetables like broccoli and related plants contain iron and calcium. Vegetables are very low in fats and calories, but ingredients added in preparation can often add them.
Grains
These foods provide complex carbohydrates, which are a good source of energy and provide much nutrition when unrefined. Examples include corn, wheat, pasta, and rice.
Fruits
In terms of food (rather than botany), fruits are the sweet-tasting seed-bearing parts of plants, or occasionally sweet parts of plants which do not bear seeds.
These include apples, oranges, grapes, bananas, etc. Fruits are low in calories and fat and are a source of natural sugars, fiber and vitamins. Processing fruit when canning or making into juices
may add sugars and remove nutrients. The fruit food group is sometimes
combined with the vegetable food group. Note that a massive number of
different plant species produce seed pods which are considered fruits in
botany, and there are a number of botanical fruits which are
conventionally not considered fruits in cuisine because they lack the characteristic sweet taste, e.g., tomatoes or avocados.
Dairy
Dairy products are produced from the milk of mammals, usually but not exclusively cattle. They include milk, yogurt and cheese. Milk and its derivative products are a rich source of dietary calcium and also provide protein, phosphorus, vitamin A, and vitamin D.
However, many dairy products are high in saturated fat and cholesterol
compared to vegetables, fruits and whole grains, which is why skimmed
products are available as an alternative.
Historically, adults were recommended to consume three cups of dairy
products per day.
More recently, evidence is mounting that dairy products have greater
levels of negative effects on health than previously thought and confer
fewer benefits. For example, recent research has shown that dairy
products are not related to stronger bones or less fractures; on the
contrary, another study showed that milk (and yogurt) consumption
results in higher bone mineral density in the hip. Overall, the majority
of research suggests that dairy has some beneficial effects on bone
health, in part because of milk's other nutrients.
Meat and beans
Meat is the tissue—usually muscle—of an animal consumed by humans. Since most parts of many animals are edible, there is a vast variety of meats. Meat is a major source of protein, as well as iron, zinc, and vitamin B12. The category of meats, poultry, and fish include beef, chicken, pork, salmon, tuna, shrimp, and eggs.
The meat group is one of the major compacted food groups in the
food guide pyramid. Since many of the same nutrients found in meat can
also be found in foods like eggs, dry beans, and nuts, such foods are typically placed in the same category as meats, as meat alternatives. These include tofu, products that resemble meat or fish but are made with soy, eggs, and cheeses. For those who do not consume meat or animal products (see Vegetarianism, veganism and Taboo food and drink), meat analogs, tofu,
beans, lentils, chickpeas, nuts and other high-protein vegetables are
also included in this group. The food guide pyramid suggests that adults
eat 2–3 servings per day. One serving of meat is 4 oz (110 g), about
the size of a deck of cards.
Oils and sweets
A
food pyramid's tip is the smallest part, so the fats and sweets in the
top of the Food Pyramid should comprise the smallest percentage of the
diet. The foods at the top of the food pyramid should be eaten sparingly
because they provide calories, but not much in the way of nutrition.
These foods include salad dressings, oils, cream, butter, margarine,
sugars, soft drinks, candies, and sweet desserts. On the 1992–2005
pyramid, the fat circle and sugar triangle are scattered throughout the
pyramid to represent the naturally-occurring fats and sugars in various
foods. The idea of this is to reduce the temptation to eat so much junk
food and excessive fats and sugars, as there is already enough fat and
sugar in the rest of the diet. For example, the triangles in the Fruit
Group represent the fact that sugar is inevitable in that group.
Criticism and controversy
USDA food pyramid
Inside the pyramid
Certain dietary choices that have been linked to heart disease, such
as an 8 oz (230 g) serving of hamburger daily, were technically
permitted under the pyramid. The pyramid also lacked differentiation
within the protein-rich group ("Meat, Poultry, Fish, Dry Beans, Eggs,
and Nuts"). The development of the US food pyramid has been influenced by food lobbyists undermining its credibility.
In April 1991, the U.S. Department of Agriculture (USDA) halted
publication of its Eating Right Pyramid, due to objections raised by
meat and dairy lobbying groups concerning the guide’s display of their
products. Despite the USDA’s explanations that the guide required
further research and testing, it was not until one year later—after its
content was supported by additional research—that the Eating Right
Pyramid was officially released. This time, even the guide’s graphic
design was altered to appease industry concerns. This incident was only
one of many in which the food industry attempted to alter federal
dietary recommendations in their own economic self-interest.
Some of the recommended quantities for the different types of
food in the old pyramid have also come under criticism for lack of
clarity. For instance, the pyramid recommends two to three servings from
the protein-rich group, but this is intended to be a maximum. The
pyramid recommends two to four fruit servings, but this is intended to
be the minimum.
The fats group as a whole have been put at the tip of the
pyramid, under the direction to eat as little as possible, which some
people have considered problematic. The guide instructs people to limit
fat intake as much as possible, which can cause health problems because
fat is essential to overall health.Research suggests that unsaturated fats aid in weight loss, reduce heart disease risk, lower blood sugar, and even lower cholesterol. Also, they are very long sustaining, and help keep blood sugar at a steady level. On top of that, these fats help brain function as well.
Several researchers have said that food and agricultural associations exert undue political power on the USDA.
Food industries, such as milk companies, have been accused of
influencing the United States Department of Agriculture into making the
colored spots on the newly created food pyramid larger for their
particular product. The milk section has been described as the easiest
to see out of the six sections of the pyramid, making individuals
believe that more milk should be consumed on a daily basis compared to
the others.
Furthermore, the inclusion of milk as a group unto itself implies that
is an essential part of a healthy diet, despite the many people who are
lactose intolerant or choose to abstain from dairy, and a number of
cultures that have historically consumed little if any dairy products. Joel Fuhrman says in his book Eat to Live that U.S. taxpayers must contribute $20 billion on price supports
to artificially reduce the price of cattle feed to benefit the dairy,
beef and veal industries, and then pay the medical bills for an
overweight population. He asks if the USDA is under the influence of the food industry, because a food pyramid based on science would have vegetables at its foundation.
These controversies prompted the creation of pyramids for specific audiences, including a Vegetarian Diet Pyramid.
The successor to the Food Pyramid called MyPlate
has also received numerous criticisms, but unlike the Food Pyramid,
which was very well known, the MyPlate program has yet to become
publicly well known, with as many as "3 out of 4 Americans [having] no
idea what the government's MyPlate dietary guide [even] is."
MyPlate
is the current nutrition guide published by the United States
Department of Agriculture, depicting a place setting with a plate and
glass divided into five food groups. It replaced the USDA's MyPyramid guide on June 2, 2011, concluding 19 years of USDA food pyramid diagrams.






.jpg)









