Discrimination against drug addicts is a form of discrimination against individuals who suffer from a drug addiction. In the process of stigmatization, drug addicts are stereotyped as having a particular set of undesirable traits, in turn causing other individuals to act in a fearful or prejudicial manner toward them. Drug use discrimination also leads to many users being secretive about drug use. As it relates to healthcare stigmatizing attitudes surrounding drug use can cause barriers to treatment uptake and engagement. In some of its manifestations, discrimination against drug addicts involves a violation of human rights.
Drug abusers are often depicted as human beings who are not
capable of staying drug free and are often addressed using derogatory
terms. The reasoning for not helping patients seek the treatments needed
are often due to the terms used to identify them, such as "crackhead"
or "junkie".
The name calling and stigma places a sense of shame for drug users for a
disease that takes control of them physically and psychologically.
Discrimination against drug abusers is very common in the workplace, and
the most familiar example happens when employers give random drug test
to see if the employee will pass it.
However, according to the Rehabilitation Act of 1973, employers are
supposed to ensure that alcoholics and other drug addicts get help and
the accommodations that they need. The lack of job opportunities and treatment for drug addicts often results in relapses or in jail.
Drug use discrimination is the unequal treatment people experience because of the drugs they use. People who use or have used illicit drugs may face discrimination in employment, welfare, housing, child custody, and travel, in addition to imprisonment, asset forfeiture, and in some cases forced labor, torture, and execution.
Though often prejudicially stereotyped as deviants and misfits, most
drug users are well-adjusted and productive members of society. Drug prohibitions may have been partly motivated by racism and other prejudice against minorities, and racial disparities have been found to exist in the enforcement and prosecution of drug laws.
Discrimination due to illicit drug use was the most commonly reported
type of discrimination among Blacks and Latinos in a 2003 study of
minority drug users in New York City, double to triple that due to race. People who use legal drugs such as tobacco and prescription medications may also face discrimination.
A report issued by the Global Commission on Drug Policy, critical of the global war on drugs, states, under "Undermining Human Rights, Fostering Discrimination":
Punitive approaches to drug policy are severely undermining human
rights in every region of the world. They lead to the erosion of civil
liberties and fair trial standards, the stigmatization of individuals
and groups – particularly women, young people, and ethnic minorities –
and the imposition of abusive and inhumane punishments.
Although still illegal at the federal level, about half of U.S.
states have legalized marijuana for medical use and several of those
states have laws, or are considering legislation, specifically
protecting medical marijuana patients from discrimination in such areas as education, employment, housing, child custody, and organ transplantation.
Drug abusers often choose the jail system because being in the
real world exposes them to the very things that made them turn to drugs. Many drug users choose jail so they can utilize the Drug Court Program.
The first drug court program was started in 1989 in Florida. The
purpose of the drug court program was to put the court's authority in
motion to reduce the drug crime rate by offering rehabilitation to drug
addicts. In 2015, up to 3,000 drug courts were available in the U.S. and
merely 120,000 defendants were being worked with per year. The overall
goal of the drug court program is to reduce the need for drugs and the
crimes that accompany them. Statistics have led researchers to believe
drug court may be an effective resolution to end drug addiction.
Motivational patterns
Drugs (especially opioids and stimulants) can change the motivational patterns of a person and lead to desocialization and degradation of personality. Acquisition of the drugs some times involves black market activities and leads to criminal social circle.
Institutional patterns
The drugs Ritalin (methylphenidate) and Adderall (amphetamine) are stimulants that are prescribed to kids with ADHD
yet in college there's an influx of this drug trafficked. These drugs
stimulate your nervous system making you awake and attentive.
Prescribing opioids to patients and related overdose has become a serious problem in the US.
Lack of objective information about drugs
An
important role in the process of discrimination is played by the lack
of objective information about drug addiction and drug addicts, caused
by legislative barriers to scientific research, the displacement of such
information by propaganda of various kinds.
Due to the lack of information about drug addiction and drug
addicts, people do not understand how an individual can become an
addict. Drug addiction has been categorized as a subcategory of mental
illness.
They are referred to as co-occurring disorders, which means if a person
is dealing with an addiction, they may also struggle with a mental
illness. Most individuals who suffer from drug dependency are nearly twice as likely to suffer from a mental illness as well.
According to the Substance Abuse and Mental Health Services
Administration, about 8.9 million adults who have an addiction also have
a psychiatric disorder. When dealing with either a mental illness or a
drug addiction some symptoms people will experience are being incapable
of controlling their own impulses and mood swings.
When an individual falls victim to drug addiction, they will
undergo the five stages of addiction which are the first use, the
continued use, tolerance, dependence, and addiction.
The first use stage, is the stage where individuals experiment with
drugs and alcohol. This is the stage where individuals will partake in
drug use because of curiosity, peer pressure, emotional problems etc.
They discover how the drug will make them feel. In the continued use
stage, individuals know how the drug makes them feel and is likely to
notice that they're not getting “high” as quickly as they use to. In the
tolerance stage, the brain and the body have adjusted to the drug and
it takes longer to get the “high” an individual is seeking. Tolerance
arrives after a period of continued use and is one of the first warning
signs of addiction. In the dependence stage, the brain becomes
accustomed to the drug and doesn't function well without it. Substance
abusers become physically ill without the use of drugs and will begin to
develop symptoms of withdrawal. This is sign that the addiction is
beginning to take hold of the individual. In the addiction stage,
individuals find it impossible to stop using drugs even if they do not
enjoy it or if their behavior has caused problems within an individual's
life.
With the increasing number of adults that suffer with an
addiction, only a few will receive treatment due to the complexity of
health care systems.
Most health care systems do not have insurance coverage for addiction
recovery and many health care providers have little to no training in
treating addiction. Some doctors do not feel comfortable treating an
addiction due to their lack of knowledge and training of the topic. This
is one of the reasons why drug dependence is difficult to recover from.
Drugs and HIV infection
Among injecting drug users, the incidence of HIV
infection is higher than among other drug addicts, however punitive and
discriminatory measures against drug addicts are not able to eliminate
either the spread of drug addiction or HIV.
Global Impact
Africa
Africa has an estimated number 28 million substance users. This number is impacted by the rising availability of injection-based drugs such as heroin, cocaine, and methamphetamines. Socio-demographic factors are often primary determinants of the health status of drug users.
These factors contribute to individual drug use behaviors such as the
sharing of needles and the solicitation of sex in exchange for police
protection or more drugs.
Nutritional status, family support, stigma/discrimination, adherence to
medication, and recovery from addiction are also impacted by these
socio-demographic factors.
Research shows that the majority of drug users transition from the use
of non-injection substances to injection substances or use both
simultaneously.
Kenya
In Kenya there is a link between injection-related discrimination, mental health, physical health, and the quality of life for those who inject drugs. The rates of discrimination are linked to higher levels of psychological distress and risk behaviors. Women in Kenya account for 1/10th of the drug users. These women tend to experience the regular discrimination faced by drug users in addition to gender related discrimination. Levels of discrimination are often higher for those that are also HIV positive.
A good friend of Socrates, once asked the Oracle at Delphi “is anyone wiser than Socrates?”
The Oracle answered “No one.”
This
greatly puzzled Socrates, since he claimed to possess no secret
information or wise insight. As far as Socrates was concerned, he was
the most ignorant man in the land.
Socrates
was determined to prove the Oracle wrong. He toured Athens up and down,
talking to its wisest and most capable people, trying to find someone
wiser than he was.
What
he found was that poets didn’t know why their words moved people,
craftsmen only knew how to master their trade and not much else, and
politicians thought they were wise but didn’t have the knowledge to back
it up.
What Socrates discovered was that none of these people
knew anything, but they all thought they did. Socrates concluded he was
wiser than them, because he at least knew that he knew nothing.
This
at least is the story of the phrase. It’s been almost 2500 years since
its longer form was initially written. In that time, it has caught a
life of its own and now has many different interpretations.
I know that I know nothing – 5 interpretations
I know that I know nothing, because I can’t trust my brain
One interpretations of the phrase asks if you can be 100% certain if a piece of information is true.
Imagine this question: “Is the Sun real?”
If
it’s day time, the answer is immediately obvious because you can simply
point your hand at the Sun and say: “Yes, of course the Sun is real.
There it is.”
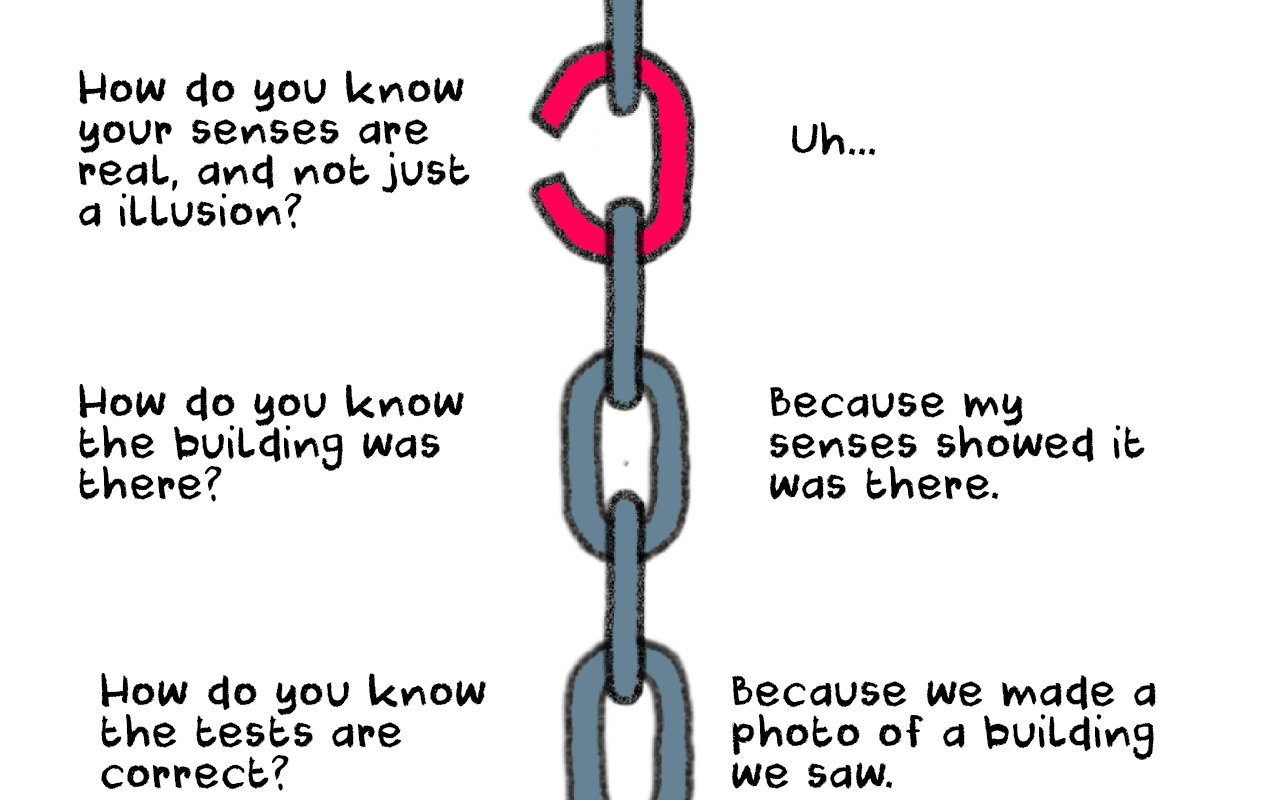
But then, you will fall into something called the infinite regress problem. This means every proof you have, must be backed up by another proof, and that proof too must be backed up by another one.
As
you go down the infinite regress, you will reach a point where you have
no proof to back up a statement. Because that one argument can’t be
proven, it then crashes all of the other statements made up to it.
French philosopher Rene Descartes went so far with the infinite regression, that he imagined the whole world was just an elaborate illusion created by an Evil Demon that wanted to trick him.
As
the Evil Demon scenario shows, the infinite regression will often go so
far down it will challenge whether any of the information entering your
brain is real or not.
Thus, if all the information you’re receiving through the senses is an illusion, then by extension you know nothing.
Counterarguments: Descartes came up with the phrase “I think, therefore I am”.
This puts a stop to the infinite regress since it’s impossible to doubt
your own existence because simply by thinking, you prove that your
consciousness exists.
Another philosophical counter argument is that some statements do not require proof in order to be called true. These are called self-evident truths, and include statements such as:
2+2 = 4
A room that contains a bed is automatically bigger than the bed.
A square contains 4 sides.
These self-evident truths act as foundations stones that allow knowledge to be built upon.
I know that I know nothing, because the physical world isn’t real
Socrates never left behind any written texts (mostly because he hated writing, saying it would damage our memory). All of the things we know about Socrates comes mostly from Plato, and to a lesser extent, Xenophon.
However,
Plato wrote his philosophy in dialogue form and always used Socrates as
the voice for his own ideas. Because of this, it’s almost impossible to
separate the true Socrates from Plato.
One
interesting interpretation of “I know that I know nothing”, is that the
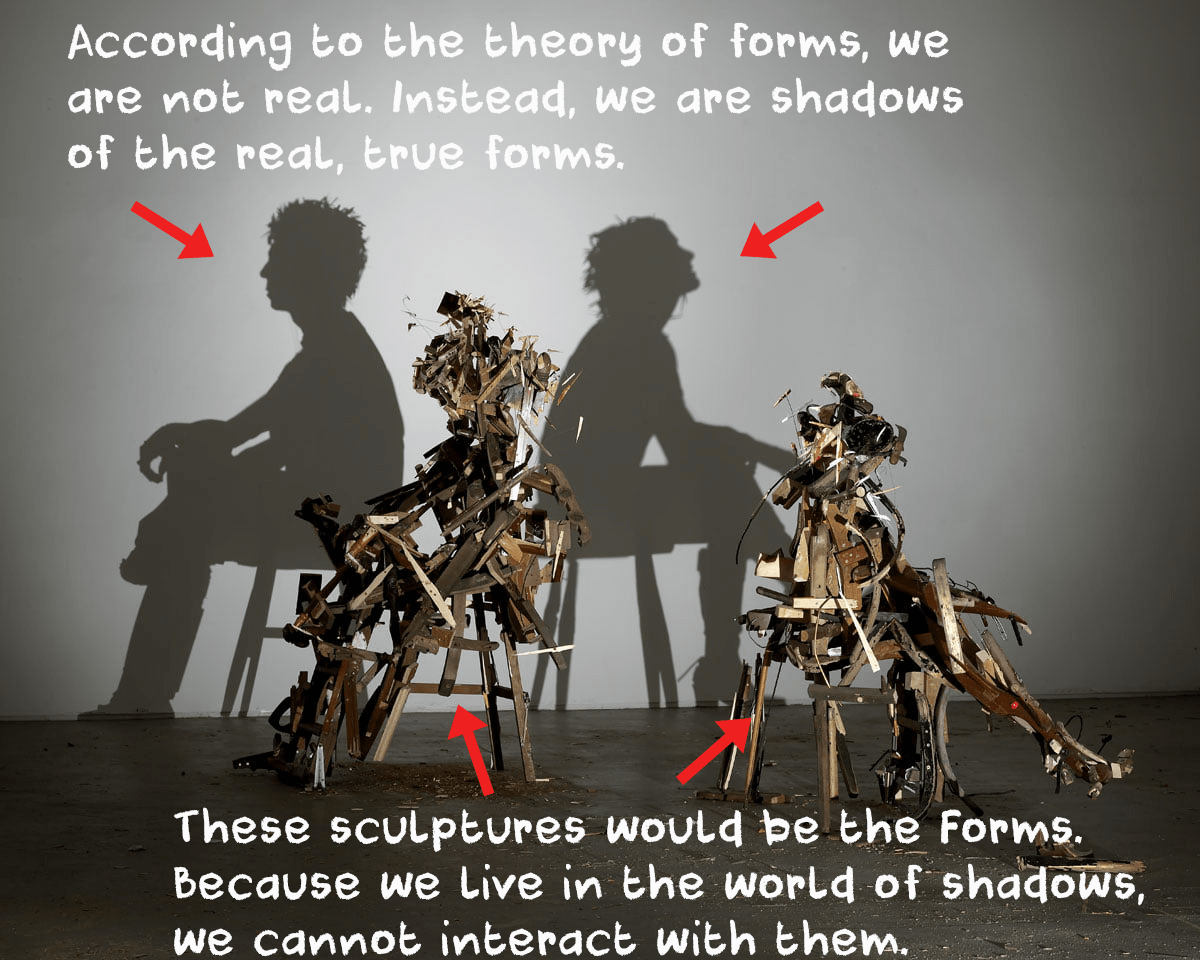
phrase could actually belong to Plato, alluding to one of his ideas: the theory of forms.
According
to theory of forms, the physical world we live in, the one where you
can read this article on a monitor or hold a glass of water, is actually
just a shadow.
The real world is that of “ideas” or “forms”.
These are non-physical essences that exist outside of our physical
world. Everything in our dimension is just an imitation, or projection
of these forms and ideas.
Another
way to think about the forms, is to compare something that exists in
the real world vs. its ideal version. For instance, imagine the perfect
apple, and then compare it to real world apples you’ve seen or eaten.
The
perfect apple (in terms of weight, crunchiness, taste, color, texture,
smell etc.) only exists in the realm of forms, and every apple you’ve
seen in real life is just a shadow, an imitation of the perfect one.
That
being said, the theory of forms does have some major limitations. One
of them is that a human living in the physical / shadow realm, you can
never know how an ideal form looks like. The best you can do is to just
think what a perfect apple, human, character, marriage etc. look like,
and try to stick to that ideal as much as possible.
You’ll never
know for sure what the ideal looks like. In this sense, “I know I know
nothing” can mean “I only know the physical realm, but I know nothing
about the real of forms”.
I know that I know nothing, because information can be uncertain
A
more straightforward interpretation is that you can never be sure if a
piece of information is correct. Viewed from this perspective, “I know
that I know nothing” becomes a motto that stops you from making hasty
judgement based on incomplete or potentially false information.
This
interpretation is also connected with the historical context in which
Socrates (or Plato) uttered the phrase. At the time, Pyrrhonism was a
philosophical school that claimed you cannot discover the truth for
anything (except the self-evident such as 2+2=4).
From the Pyrrhonist point of view,
you cannot say for sure if a statement is correct or false because
there will always be arguments for and against that will cancel each
other out.
For instance, imagine the color green.
A Pyrrhonist would argue that you cannot be sure this is the color green because:
Animals might perceive this color differently.
Other people might perceive the color differently because of different lighting, color blindness etc.
A non-philosopher would just say “it’s green dammit, what more do you need?” and close the problem.
What
makes Pyrrhonists different is that instead of saying “yes this is a
color, and that color is green”, they will simply say “yes, this is a
color, but I’m not sure which so I’d rather not say”.
For
Pyrrhonists however, such a position was not just a philosophical
exercise. They extended this way of thinking to their entire lives so it
became a mindset called epoché,
translated as suspension of judgement. This suspension of judgement
then led to the mental state of ataraxia, often translated as
tranquility.
From the Pyrrhonist point of view, people cannot
achieve happiness because their minds are in a state of conflict by
having to come to conclusions in the face of contradictory arguments.
As
a result, Pyrrhonists chose to suspend their judgement on all problems
that were not self-evident, hoping that thus they will achieve true
happiness.
Ultimately, from the Pyrrhonist perspective, “I know that I know nothing” can mean “truth cannot be discovered”.
I know that I know nothing – the paradox
A
more conventional approach to the phrase is to simply view it as a
self-referential paradox. The most well-known self-referential paradox
is the phrase “this sentence is a lie”.
These pair of drawing hands by M.C. Escher self-reference each other
When
it comes to science and knowledge, paradoxes function as indications
that a logical argument is flawed, or that our way of thinking will
produce bad results.
A more interesting overview of self-referencing paradoxes is the book Gödel, Escher, Bach: An Eternal Golden Braid
by Douglas Hofstader. This book explores how meaningless elements,
(such as carbon, hydrogen etc.) form systems, and how these systems can
then become self-aware through a process of self-reference.
I know that I know nothing – a motto of humility
Socrates lived in a world that had accumulated very little knowledge.
As
a fun fact, Aristotle (who was born some 15 years after Socrates died),
was said to be the last man on Earth to have known every ounce of
knowledge available at the time.
From the perspective of Socrates,
any knowledge or information he did have was likely to be insignificant
(or even completely false) compared to how much was left to be
discovered.
From
such a position, it’s easier to say “I know that I know nothing” rather
than the more technical truth: “I only know the tiniest bit of
knowledge, and even that is probably incorrect”.
The same
principle still applies to us, if we compare ourselves to humans living
200-300 years in the future. And unlike Socrates, we have a giant wealth
of information to dive in whenever we want.
Psychoactive substances often bring about subjective (although
these may be objectively observed) changes in consciousness and mood
that the user may find rewarding and pleasant (e.g., euphoria or a sense of relaxation) or advantageous (e.g. increased alertness) and are thus reinforcing. Substances which are both rewarding and positively reinforcing have the potential to induce a state of addiction – compulsive drug use despite negative consequences. In addition, sustained use of some substances may produce physical or psychological dependence or both, associated with somatic or psychological-emotional withdrawal states respectively. Drug rehabilitation attempts to reduce addiction, through a combination of psychotherapy,
support groups, and other psychoactive substances. Conversely, certain
psychoactive drugs may be so unpleasant that the person will never use
the substance again. This is especially true of certain deliriants (e.g. Jimson weed), powerful dissociatives (e.g. Salvia divinorum), and classic psychedelics (e.g. LSD, psilocybin), in the form of a "bad trip".
Psychoactive drug misuse, dependence and addiction have resulted
in legal measures and moral debate. Governmental controls on
manufacture, supply and prescription attempt to reduce problematic
medical drug use. Ethical concerns
have also been raised about over-use of these drugs clinically, and
about their marketing by manufacturers. Popular campaigns to
decriminalize or legalize certain recreational drug use (e.g. cannabis) are also ongoing.
History
Alcohol is a widely used and abused psychoactive drug. The global alcoholic drinks market was expected to exceed $1 trillion in 2013. Beer is the third-most popular drink overall, after water and tea.
Psychoactive drug use can be traced to prehistory.
There is archaeological evidence of the use of psychoactive substances
(mostly plants) dating back at least 10,000 years, and historical
evidence of cultural use over the past 5,000 years. The chewing of coca leaves, for example, dates back over 8,000 years ago in Peruvian society.
Medicinal use is one important facet of psychoactive drug usage.
However, some have postulated that the urge to alter one's consciousness
is as primary as the drive to satiate thirst, hunger or sexual desire.[7]
Supporters of this belief contend that the history of drug use and even
children's desire for spinning, swinging, or sliding indicate that the
drive to alter one's state of mind is universal.
One of the first people to articulate this point of view, set aside from a medicinal context, was American author Fitz Hugh Ludlow (1836–1870) in his book The Hasheesh Eater (1857):
[D]rugs
are able to bring humans into the neighborhood of divine experience and
can thus carry us up from our personal fate and the everyday
circumstances of our life into a higher form of reality. It is, however,
necessary to understand precisely what is meant by the use of drugs. We
do not mean the purely physical craving...That of which we speak is
something much higher, namely the knowledge of the possibility of the
soul to enter into a lighter being, and to catch a glimpse of deeper
insights and more magnificent visions of the beauty, truth, and the
divine than we are normally able to spy through the cracks in our prison
cell. But there are not many drugs which have the power of stilling
such craving. The entire catalog, at least to the extent that research
has thus far written it, may include only opium, hashish, and in rarer
cases alcohol, which has enlightening effects only upon very particular characters.
This relationship is not limited to humans. A number of animals
consume different psychoactive plants, animals, berries and even
fermented fruit, becoming intoxicated, such as cats after consuming catnip. Traditional legends of sacred plants often contain references to animals that introduced humankind to their use. Animals and psychoactive plants appear to have co-evolved, possibly explaining why these chemicals and their receptors exist within the nervous system.
During the 20th century, many governments across the world
initially responded to the use of recreational drugs by banning them and
making their use, supply, or trade a criminal offense. A notable
example of this was Prohibition
in the United States, where alcohol was made illegal for 13 years.
However, many governments, government officials and persons in law
enforcement have concluded that illicit drug use cannot be sufficiently
stopped through criminalization. Organizations such as Law Enforcement
Against Prohibition (LEAP) have come to such a conclusion, believing:
[T]he existing drug policies have
failed in their intended goals of addressing the problems of crime, drug
abuse, addiction, juvenile drug use, stopping the flow of illegal drugs
into this country and the internal sale and use of illegal drugs. By
fighting a war on drugs the government has increased the problems of
society and made them far worse. A system of regulation rather than
prohibition is a less harmful, more ethical and a more effective public
policy.
In some countries, there has been a move toward harm
reduction by health services, where the use of illicit drugs is neither
condoned nor promoted, but services and support are provided to ensure
users have adequate factual information readily available, and that the
negative effects of their use be minimized. Such is the case of
Portuguese drug policy of decriminalization, which achieved its primary
goal of reducing the adverse health effects of drug abuse.
Purposes
Psychoactive
substances are used by humans for a number of different purposes to
achieve a specific end. These uses vary widely between cultures. Some
substances may have controlled or illegal uses while others may have
shamanic purposes, and still others are used medicinally. Other examples
would be social drinking, nootropic, or sleep aids. Caffeine
is the world's most widely consumed psychoactive substance, but unlike
many others, it is legal and unregulated in nearly all jurisdictions. In
North America, 90% of adults consume caffeine daily.
Psychoactive drugs are divided into different groups according to
their pharmacological effects. Commonly used psychoactive drugs and
groups:
Depressants ("downers"), including sedatives, hypnotics, and opioids.
This category includes all of the calmative, sleep-inducing,
anxiety-reducing, anesthetizing substances, which sometimes induce
perceptual changes, such as dream images, and also often evoke feelings
of euphoria.
Hallucinogens, including psychedelics, dissociatives and deliriants.
This category encompasses all those substances that produce distinct
alterations in perception, sensation of space and time, and emotional
states
General anesthetics
are a class of psychoactive drug used on people to block physical pain
and other sensations. Most anesthetics induce unconsciousness, allowing
the person to undergo medical procedures like surgery without the feelings of physical pain or emotional trauma. To induce unconsciousness, anesthetics affect the GABA and NMDA systems. For example, propofol is a GABA agonist, and ketamine is an NMDA receptor antagonist.
Psychiatric medications are psychoactive drugs prescribed for the management of mental and emotional disorders, or to aid in overcoming challenging behavior. There are six major classes of psychiatric medications:
Exposure to psychoactive drugs can cause changes to the brain
that counteract or augment some of their effects; these changes may be
beneficial or harmful. However, there is a significant amount of
evidence that relapse rate of mental disorders negatively corresponds
with length of properly followed treatment regimens (that is, relapse
rate substantially declines over time), and to a much greater degree
than placebo.
Recreation
Many psychoactive substances are used for their mood and perception
altering effects, including those with accepted uses in medicine and
psychiatry. Examples of psychoactive substances include caffeine, alcohol, cocaine, LSD, nicotine and cannabis. Classes of drugs frequently used recreationally include:
Hypnotics, which depress the central nervous system.
Opioid analgesics, which also depress the central nervous system. These are used recreationally because of their euphoric effects.
Inhalants,
in the forms of gas aerosols, or solvents, which are inhaled as a vapor
because of their stupefying effects. Many inhalants also fall into the
above categories (such as nitrous oxide which is also an analgesic).
In some modern and ancient cultures, drug usage is seen as a status symbol. Recreational drugs are seen as status symbols in settings such as at nightclubs and parties. For example, in ancient Egypt, gods were commonly pictured holding hallucinogenic plants.
Because there is controversy about regulation of recreational drugs, there is an ongoing debate about drug prohibition. Critics of prohibition believe that regulation of recreational drug use is a violation of personal autonomy and freedom. In the United States, critics have noted that prohibition or regulation of recreational and spiritual drug use might be unconstitutional, and causing more harm than is prevented.
Ritual and spiritual
Timothy Leary was a leading proponent of spiritual hallucinogen use.
Certain psychoactives, particularly hallucinogens, have been used for
religious purposes since prehistoric times. Native Americans have used peyote cacti containing mescaline for religious ceremonies for as long as 5700 years. The muscimol-containing Amanita muscaria mushroom was used for ritual purposes throughout prehistoric Europe.
The use of entheogens for religious purposes resurfaced in the West during the counterculture movements of the 1960s and 70s. Under the leadership of Timothy Leary, new spiritual and intention-based movements began to use LSD
and other hallucinogens as tools to access deeper inner exploration. In
the United States, the use of peyote for ritual purposes is protected
only for members of the Native American Church, which is allowed to cultivate and distribute peyote.
However, the genuine religious use of peyote, regardless of one's
personal ancestry, is protected in Colorado, Arizona, New Mexico,
Nevada, and Oregon.
Military
Psychoactive drugs have been used in military applications as non-lethal weapons.
Both military and civilian American intelligence officials are
known to have used psychoactive drugs while interrogating captives
apprehended in its War on Terror. In July 2012, Jason Leopold and Jeffrey Kaye, psychologists and human rights workers, had a Freedom of Information Act request fulfilled that confirmed that the use of psychoactive drugs during interrogation was a long-standing
practice.
Captives and former captives had been reporting medical staff
collaborating with interrogators to drug captives with powerful
psychoactive drugs prior to interrogation since the very first captives'
release.
In May 2003, recently released Pakistani captiveSha Mohammed Alikhel described the routine use of psychoactive drugs in the Guantanamo Bay detention center. He said that Jihan Wali, a captive kept in a nearby cell, was rendered catatonic through the use of these drugs.
The military justice system has also been known to use psychoactive drugs to obtain a conviction. (U.S. vs. Juillerat)
Additionally, militaries worldwide have used or are using various psychoactive drugs to improve performance of soldiers by suppressing hunger, increasing the ability to sustain effort without food, increasing and lengthening wakefulness and concentration, suppressing fear, reducing empathy, and improving reflexes and memory-recall among other things.
Route of administration
Psychoactive drugs are administered via oral ingestion as a tablet, capsule, powder, liquid, and beverage; via injection by subcutaneous, intramuscular, and intravenous route; via rectum by suppository and enema; and via inhalation by smoking, vaporization and insufflation ("snorting"). The efficiency of each method of administration varies from drug to drug.
The
theory of dosage, set, and setting is a useful model in dealing with
the effects of psychoactive substances, especially in a controlled
therapeutic setting as well as in recreational use. Dr. Timothy Leary, based on his own experiences and systematic observations on psychedelics, developed this theory along with his colleagues Ralph Metzner, and Richard Alpert (Ram Dass) in the 1960s.
Dosage
The first factor, dosage, has been a truism since ancient times, or at least since Paracelsus
who said, "Dose makes the poison." Some compounds are beneficial or
pleasurable when consumed in small amounts, but harmful, deadly, or
evoke discomfort in higher doses.
Set
The set is the internal attitudes and constitution of the person,
including their expectations, wishes, fears, and sensitivity to the
drug. This factor is especially important for the hallucinogens, which
have the ability to make conscious experiences out of the unconscious.
In traditional cultures, set is shaped primarily by the worldview,
health and genetic characteristics that all the members of the culture
share.
Setting
The third aspect is setting, which pertains to the surroundings, the place, and the time in which the experiences transpire.
This theory clearly states that the effects are equally the
result of chemical, pharmacological, psychological, and physical
influences. The model that Timothy Leary proposed applied to the
psychedelics, although it also applies to other psychoactives.[41]
Effects
Illustration of the major elements of neurotransmission. Depending on its method of action, a psychoactive substance may block the receptors on the post-synaptic neuron (dendrite), or block reuptake or affect neurotransmitter synthesis in the pre-synaptic neuron (axon).
Psychoactive drugs operate by temporarily affecting a person's
neurochemistry, which in turn causes changes in a person's mood,
cognition, perception and behavior. There are many ways in which
psychoactive drugs can affect the brain. Each drug has a specific action
on one or more neurotransmitter or neuroreceptor in the brain.
Drugs that increase activity in particular neurotransmitter systems are called agonists. They act by increasing the synthesis of one or more neurotransmitters, by reducing its reuptake from the synapses,
or by mimicking the action by binding directly to the postsynaptic
receptor. Drugs that reduce neurotransmitter activity are called antagonists, and operate by interfering with synthesis or blocking postsynaptic receptors so that neurotransmitters cannot bind to them.
Exposure to a psychoactive substance can cause changes in the structure and functioning of neurons, as the nervous system tries to re-establish the homeostasis disrupted by the presence of the drug (see also, neuroplasticity).
Exposure to antagonists for a particular neurotransmitter can increase
the number of receptors for that neurotransmitter or the receptors
themselves may become more responsive to neurotransmitters; this is
called sensitization.
Conversely, overstimulation of receptors for a particular
neurotransmitter may cause a decrease in both number and sensitivity of
these receptors, a process called desensitization or tolerance.
Sensitization and desensitization are more likely to occur with
long-term exposure, although they may occur after only a single
exposure. These processes are thought to play a role in drug dependence
and addiction. Physical dependence
on antidepressants or anxiolytics may result in worse depression or
anxiety, respectively, as withdrawal symptoms. Unfortunately, because clinical depression (also called major depressive disorder) is often referred to simply as depression, antidepressants are often requested by and prescribed for patients who are depressed, but not clinically depressed.
Affected neurotransmitter systems
The
following is a brief table of notable drugs and their primary
neurotransmitter, receptor or method of action. Many drugs act on more
than one transmitter or receptor in the brain.
Comparison
of the perceived harm for various psychoactive drugs from a poll among
medical psychiatrists specialized in addiction treatment (David Nutt et al. 2007).
Psychoactive drugs are often associated with addiction or drug dependence. Dependence can be divided into two types: psychological dependence, by which a user experiences negative psychological or emotional withdrawal symptoms (e.g., depression) and physical dependence, by which a user must use a drug to avoid physically uncomfortable or even medically harmful physical withdrawal symptoms. Drugs that are both rewarding and reinforcing are addictive; these properties of a drug are mediated through activation of the mesolimbic dopamine pathway, particularly the nucleus accumbens. Not all addictive drugs are associated with physical dependence, e.g., amphetamine, and not all drugs that produce physical dependence are addictive drugs, e.g., caffeine.
Many professionals, self-help groups, and businesses specialize in drug rehabilitation,
with varying degrees of success, and many parents attempt to influence
the actions and choices of their children regarding psychoactives.
Common forms of rehabilitation include psychotherapy, support groups and pharmacotherapy, which uses psychoactive substances to reduce cravings and physiological withdrawal symptoms while a user is going through detox. Methadone, itself an opioid and a psychoactive substance, is a common treatment for heroin addiction, as is another opioid, buprenorphine. Recent research on addiction has shown some promise in using psychedelics such as ibogaine to treat and even cure drug addictions, although this has yet to become a widely accepted practice.
The legality of psychoactive drugs has been controversial through most of recent history; the Second Opium War and Prohibition
are two historical examples of legal controversy surrounding
psychoactive drugs. However, in recent years, the most influential
document regarding the legality of psychoactive drugs is the Single Convention on Narcotic Drugs, an international treaty signed in 1961 as an Act of the United Nations. Signed by 73 nations including the United States, the USSR, India, and the United Kingdom,
the Single Convention on Narcotic Drugs established Schedules for the
legality of each drug and laid out an international agreement to fight
addiction to recreational drugs by combatting the sale, trafficking, and use of scheduled drugs.
All countries that signed the treaty passed laws to implement these
rules within their borders. However, some countries that signed the
Single Convention on Narcotic Drugs, such as the Netherlands, are more lenient with their enforcement of these laws.
In the United States, the Food and Drug Administration (FDA) has authority over all drugs, including psychoactive drugs. The FDA regulates which psychoactive drugs are over the counter and which are only available with a prescription.
However, certain psychoactive drugs, like alcohol, tobacco, and drugs
listed in the Single Convention on Narcotic Drugs are subject to
criminal laws. The Controlled Substances Act of 1970 regulates the recreational drugs outlined in the Single Convention on Narcotic Drugs. Alcohol is regulated by state governments, but the federal National Minimum Drinking Age Act penalizes states for not following a national drinking age. Tobacco is also regulated by all fifty state governments.
Most people accept such restrictions and prohibitions of certain drugs,
especially the "hard" drugs, which are illegal in most countries.
In the medical context, psychoactive drugs as a treatment for
illness is widespread and generally accepted. Little controversy exists
concerning over the counter psychoactive medications in antiemetics and antitussives.
Psychoactive drugs are commonly prescribed to patients with psychiatric
disorders. However, certain critics believe that certain prescription
psychoactives, such as antidepressants and stimulants, are overprescribed and threaten patients' judgement and autonomy.





















.svg)




