In its broadest sense, social vulnerability is one dimension of vulnerability to multiple stressors and shocks, including abuse, social exclusion and natural hazards. Social vulnerability refers to the inability of people,
organizations, and societies to withstand adverse impacts from multiple
stressors to which they are exposed. These impacts are due in part to
characteristics inherent in social interactions, institutions, and systems of cultural values.
Because it is most apparent when calamity occurs, many studies of social vulnerability are found in risk management literature.
The concept of social vulnerability emerged most recently within
the discourse on natural hazards and disasters. To date no one
definition has been agreed upon. Similarly, multiple theories of social
vulnerability exist.
Most work conducted so far focuses on empirical observation and
conceptual models. Thus, current social vulnerability research is a middle range theory
and represents an attempt to understand the social conditions that
transform a natural hazard (e.g. flood, earthquake, mass movements etc.)
into a social disaster. The concept emphasizes two central themes:
Both the causes and the phenomenon of disasters are defined by
social processes and structures. Thus it is not only a geo- or
biophysical hazard, but rather the social context that is taken into
account to understand “natural” disasters (Hewitt 1983).
Although different groups of a society may share a similar exposure
to a natural hazard, the hazard has varying consequences for these
groups, since they have diverging capacities and abilities to handle the
impact of a hazard.
Taking a structuralist view, Hewitt (1997, p143) defines vulnerability as being:
...essentially about the human ecology of endangerment...and is
embedded in the social geography of settlements and lands uses, and the
space of distribution of influence in communities and political
organisation.
this is in contrast to the more socially focused view of Blaikie et al. (1994, p9) who define vulnerability as the:
...set of characteristics of a group or individual in terms of their
capacity to anticipate, cope with, resist and recover from the impact of
a natural hazard. It involves a combination of factors that determine
the degree to which someone's life and livelihood is at risk by a
discrete and identifiable event in nature or society.
History of the concept
In
the 1970s the concept of vulnerability was introduced within the
discourse on natural hazards and disaster by O´Keefe, Westgate and
Wisner (O´Keefe, Westgate et al. 1976). In “taking the naturalness out
of natural disasters” these authors insisted that socio-economic
conditions are the causes for natural disasters. The work illustrated by
means of empirical data that the occurrence of disasters increased over
the last 50 years, paralleled by an increasing loss of life. The work
also showed that the greatest losses of life concentrate in
underdeveloped countries, where the authors concluded that vulnerability
is increasing.
Chambers put these empirical findings on a conceptual level and
argued that vulnerability has an external and internal side: People are
exposed to specific natural and social risk. At the same time people
possess different capacities to deal with their exposure by means of
various strategies of action (Chambers 1989). This argument was again
refined by Blaikie, Cannon, Davis and Wisner, who went on to develop the
Pressure and Release Model (PAR) (see below). Watts and Bohle argued
similarly by formalizing the “social space of vulnerability”, which is
constituted by exposure, capacity and potentiality (Watts and Bohle
1993).
Susan Cutter
developed an integrative approach (hazard of place), which tries to
consider both multiple geo- and biophysical hazards on the one hand as
well as social vulnerabilities on the other hand (Cutter, Mitchell et
al. 2000). Recently, Oliver-Smith grasped the nature-culture dichotomy
by focusing both on the cultural construction of the
people-environment-relationship and on the material production of
conditions that define the social vulnerability of people (Oliver-Smith
and Hoffman 2002).
Research on social vulnerability to date has stemmed from a
variety of fields in the natural and social sciences. Each field has
defined the concept differently, manifest in a host of definitions and
approaches (Blaikie, Cannon et al. 1994; Henninger 1998; Frankenberger,
Drinkwater et al. 2000; Alwang, Siegel et al. 2001; Oliver-Smith 2003;
Cannon, Twigg et al. 2005). Yet some common threads run through most of
the available work.
Within society
Although
considerable research attention has examined components of biophysical
vulnerability and the vulnerability of the built environment
(Mileti, 1999), we currently know the least about the social aspects of
vulnerability (Cutter et al., 2003). Socially created vulnerabilities
are largely ignored, mainly due to the difficulty in quantifying them.
Social vulnerability is created through the interaction of social forces
and multiple stressors, and resolved through social (as opposed to
individual) means. While individuals within a socially vulnerable
context may break through the “vicious cycle,” social vulnerability
itself can persist because of structural—i.e. social and
political—influences that reinforce vulnerability.
Social vulnerability is partially the product of social
inequalities—those social factors that influence or shape the
susceptibility of various groups to harm and that also govern their
ability to respond (Cutter et al., 2003). It is, however, important to
note that social vulnerability is not registered by exposure to hazards
alone, but also resides in the sensitivity and resilience of the system
to prepare, cope and recover from such hazards (Turner et al., 2003).
However, it is also important to note, that a focus limited to the
stresses associated with a particular vulnerability analysis is also
insufficient for understanding the impact on and responses of the
affected system or its components (Mileti, 1999; Kaperson et al., 2003;
White & Haas, 1974). These issues are often underlined in attempts
to model the concept (see Models of Social Vulnerability).
Models
Risk-Hazard
(RH) model (diagram after Turner et al., 2003), showing the impact of a
hazard as a function of exposure and sensitivity. The chain sequence
begins with the hazard, and the concept of vulnerability is noted
implicitly as represented by white arrows.
Two of the principal archetypal reduced-form models of social
vulnerability are presented, that have informed vulnerability analysis:
the Risk-Hazard (RH) model and the Pressure and Release model.
Risk-Hazard (RH) Model
Initial
RH models sought to understand the impact of a hazard as a function of
exposure to the hazardous event and the sensitivity of the entity
exposed (Turner et al., 2003). Applications of this model in
environmental and climate impact assessments generally emphasised
exposure and sensitivity to perturbations and stressors (Kates, 1985;
Burton et al., 1978) and worked from the hazard to the impacts (Turner
et al., 2003). However, several inadequacies became apparent.
Principally, it does not treat the ways in which the systems in question
amplify or attenuate the impacts of the hazard (Martine & Guzman,
2002). Neither does the model address the distinction among exposed
subsystems and components that lead to significant variations in the
consequences of the hazards, or the role of political economy in shaping
differential exposure and consequences (Blaikie et al., 1994, Hewitt,
1997). This led to the development of the PAR model.
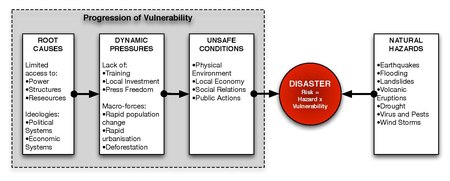
Pressure and Release (PAR) Model
Pressure
and Release (PAR) model after Blaikie et al. (1994) showing the
progression of vulnerability. The diagram shows a disaster as the
intersection between socio-economic pressures on the left and physical
exposures (natural hazards) on the right
The PAR model understands a disaster as the intersection between
socio-economic pressure and physical exposure. Risk is explicitly
defined as a function of the perturbation, stressor, or stress and the
vulnerability of the exposed unit (Blaikie et al, 1994). In this way, it
directs attention to the conditions that make exposure unsafe, leading
to vulnerability and to the causes creating these conditions. Used
primarily to address social groups facing disaster events, the model
emphasises distinctions in vulnerability by different exposure units
such as social class and ethnicity. The model distinguishes between
three components on the social side: root causes, dynamic pressures and
unsafe conditions, and one component on the natural side, the natural
hazards itself. Principal root causes include “economic, demographic and
political processes”, which affect the allocation and distribution of
resources between different groups of people. Dynamic Pressures
translate economic and political processes in local circumstances (e.g.
migration patterns). Unsafe conditions are the specific forms in which
vulnerability is expressed in time and space, such as those induced by
the physical environment, local economy or social relations (Blaikie,
Cannon et al. 1994).
Although explicitly highlighting vulnerability, the PAR model
appears insufficiently comprehensive for the broader concerns of
sustainability science (Turner et al., 2003). Primarily, it does not
address the coupled human environment system in the sense of considering
the vulnerability of biophysical subsystems (Kasperson et al, 2003) and
it provides little detail on the structure of the hazard's causal
sequence. The model also tends to underplay feedback beyond the system
of analysis that the integrative RH models included (Kates, 1985).
Criticism
Some
authors criticise the conceptualisation of social vulnerability for
overemphasising the social, political and economical processes and
structures that lead to vulnerable conditions. Inherent in such a view
is the tendency to understand people as passive victims (Hewitt 1997)
and to neglect the subjective and intersubjective interpretation and
perception of disastrous events. Bankoff criticises the very basis of
the concept, since in his view it is shaped by a knowledge system that
was developed and formed within the academic environment of western
countries and therefore inevitably represents values and principles of
that culture. According to Bankoff the ultimate aim underlying this
concept is to depict large parts of the world as dangerous and hostile
to provide further justification for interference and intervention
(Bankoff 2003).
Current and future research
Social vulnerability research has become a deeply interdisciplinary
science, rooted in the modern realization that humans are the causal
agents of disasters – i.e., disasters are never natural, but a
consequence of human behavior. The desire to understand geographic,
historic, and socio-economic characteristics of social vulnerability
motivates much of the research being conducted around the world today.
Two principal goals are currently driving the field of social vulnerability research:
The design of models which explain vulnerability and the root causes which create it, and
The development of indicators and indexes which attempt to map vulnerability over time and space (Villágran de León 2006).
The temporal and spatial aspects of vulnerability science are
pervasive, particularly in research that attempts to demonstrate the
impact of development on social vulnerability. Geographic Information Systems (GIS)
are increasingly being used to map vulnerability, and to better
understand how various phenomena (hydrological, meteorological,
geophysical, social, political and economic) effect human populations.
Researchers have yet to develop reliable models capable of
predicting future outcomes based upon existing theories and data.
Designing and testing the validity of such models, particularly at the
sub-national scale at which vulnerability reduction takes place, is
expected to become a major component of social vulnerability research in
the future.
An even greater aspiration in social vulnerability research is
the search for one, broadly applicable theory, which can be applied
systematically at a variety of scales, all over the world. Climate
change scientists, building engineers, public health specialists, and
many other related professions have already achieved major strides in
reaching common approaches. Some social vulnerability scientists argue
that it is time for them to do the same, and they are creating a variety
of new forums in order to seek a consensus on common frameworks,
standards, tools, and research priorities. Many academic, policy, and
public/NGO organizations promote a globally applicable approach in
social vulnerability science and policy (see section 5 for links to some
of these institutions).
Disasters often expose pre-existing societal inequalities that
lead to disproportionate loss of property, injury, and death (Wisner,
Blaikie, Cannon, & Davis, 2004). Some disaster researchers argue
that particular groups of people are placed disproportionately at-risk
to hazards. Minorities, immigrants, women, children, the poor, as well
as people with disabilities are among those have been identified as
particularly vulnerable to the impacts of disaster (Cutter et al., 2003;
Peek, 2008; Stough, Sharp, Decker & Wilker, 2010).
Since 2005, the Spanish Red Cross has developed a set of
indicators to measure the multi-dimensional aspects of social
vulnerability. These indicators are generated through the statistical
analysis of more than 500 thousand people who are suffering of economic
strain and social vulnerability, and who have a personal record
containing 220 variables at the Red Cross database. An Index on Social
Vulnerability in Spain is produced annually, both for adults and for
children.
Collective vulnerability
Collective
vulnerability is a state in which the integrity and social fabric of a
community is or was threatened through traumatic events or repeated
collective violence. In addition, according to the collective vulnerability hypothesis,
shared experience of vulnerability and the loss of shared normative
references can lead to collective reactions aimed to reestablish the
lost norms and trigger forms of collective resilience.
This theory has been developed by social psychologists to study
the support for human rights. It is rooted in the consideration that
devastating collective events are sometimes followed by claims for
measures that may prevent that similar event will happen again. For
instance, the Universal Declaration of Human Rights
was a direct consequence of World War II horrors. Psychological
research by Willem Doise and colleagues shows indeed that after people
have experienced a collective injustice, they are more likely to support
the reinforcement of human rights.
Populations who collectively endured systematic human rights violations
are more critical of national authorities and less tolerant of rights
violations. Some analyses performed by Dario Spini, Guy Elcheroth and Rachel Fasel
on the Red Cross' “People on War” survey shows that when individuals
have direct experience with the armed conflict are less keen to support
humanitarian norms. However, in countries in which most of the social
groups in conflict share a similar level of victimization, people
express more the need for reestablishing protective social norms as the
human rights, no matter the magnitude of the conflict.
Research opportunities and challenges
Research
on social vulnerability is expanding rapidly to fill the research and
action gaps in this field. This work can be characterized in three major
groupings, including research, public awareness, and policy. The
following issues have been identified as requiring further attention to
understand and reduce social vulnerability (Warner and Loster 2006):
Research
1. Foster a common understanding of social vulnerability – its definition(s), theories, and measurement approaches.
2. Aim for science that produces tangible and applied outcomes.
3. Advance tools and methodologies to reliably measure social vulnerability.
Public awareness
4. Strive for better understanding of nonlinear relationships and
interacting systems (environment, social and economic, hazards), and
present this understanding coherently to maximize public understanding.
5. Disseminate and present results in a coherent manner for the
use of lay audiences. Develop straight forward information and practical
education tools.
6. Recognize the potential of the media as a bridging device between science and society.
Policy
7. Involve local communities and stakeholders considered in vulnerability studies.
8. Strengthen people's ability to help themselves, including an (audible) voice in resource allocation decisions.
9. Create partnerships that allow stakeholders from local, national, and international levels to contribute their knowledge.
10. Generate individual and local trust and ownership of vulnerability reduction efforts.
Debate and ongoing discussion surround the causes and possible
solutions to social vulnerability. In cooperation with scientists and
policy experts worldwide, momentum is gathering around practice-oriented
research on social vulnerability. In the future, links will be
strengthened between ongoing policy and academic work to solidify the
science, consolidate the research agenda, and fill knowledge gaps about
causes of and solutions for social vulnerability.
According to many definitions, a disability or functional impairment is an impairment that may be cognitive, developmental, intellectual, mental, physical, sensory,
or some combination of these. Other definitions describe disability as
the societal disadvantage arising from such impairments. Disability
substantially affects a person's life activities and may be present from
birth or occur during a person's lifetime.
Disabilities is an umbrella term,
covering impairments, activity limitations, and participation
restrictions. An impairment is a problem in body function or structure;
an activity limitation is a difficulty encountered by an individual in
executing a task or action; while a participation restriction is a
problem experienced by an individual in involvement in life situations.
Disability is thus not just a health problem. It is a complex
phenomenon, reflecting the interaction between features of a person’s
body and features of the society in which he or she lives.
Disability is a contested concept, with different meanings in different communities. The term disability
may be used to refer to physical or mental attributes that some
institutions, particularly medicine, view as needing to be fixed (the medical model); it may also refer to limitations imposed on people by the constraints of an ableist society (the social model); or the term may serve to refer to the identity of disabled people. Physiological functional capacity
(PFC) is a measure of an individual's performance level that gauges
one's ability to perform the physical tasks of daily life and the ease
with which these tasks are performed. PFC declines with advancing age to result in frailty, cognitive disorders, or physical disorders, all of which may lead to labeling individuals as disabled.
Terminology
Handicapped
Handicap has been disparaged as a result of false folk etymology that claims it is a reference to begging. The term is actually derived from an old game, Hand-i'-cap, in which two players trade possessions and a third, neutral person judges the difference of value between the possessions. The concept of a neutral person evening up the odds was extended to handicap racing
in the mid-18th century. In handicap racing, horses carry different
weights based on the umpire's estimation of what would make them run
equally. The use of the term to describe a person with a disability – by
extension from handicap racing, a person carrying a heavier burden than
normal – appeared in the early 20th century.
Access
The ability to go places and do things. People with certain types
of disabilities struggle to get equal access to some things in society.
For example, a blind person cannot read printed paper voting ballots, and therefore does not have access to voting that requires paper ballots.
Accommodation
A change that improves access. For example, if voting ballots are available in Braille or on a text-to-speech
machine, or if another person read the ballot to the blind person and
recorded the choices, then the blind person would have access to voting.
Types
There are
many different types of disability. Often, disability is understood as a
situation that produces a long-term impairment that affects activities of daily living, such as eating, walking, and maintaining personal hygiene.
Acquired disability
A disability that the person was not born with. For example, Alzheimer's disease produces an acquired disability in previously healthy people.
Contemporary understandings of disability derive from concepts that arose during the West's scientific Enlightenment; prior to the Enlightenment, physical differences were viewed through a different lens.
During the Middle Ages,
madness and other conditions were thought to be caused by demons. They
were also thought to be part of the natural order, especially during and
in the fallout of the Plague, which wrought impairments throughout the general population. In the early modern period
there was a shift to seeking biological causes for physical and mental
differences, as well as heightened interest in demarcating categories:
for example, Ambroise Pare, in the sixteenth century, wrote of
"monsters", "prodigies", and "the maimed". The European Enlightenment's
emphases on knowledge derived from reason and on the value of natural
science to human progress helped spawn the birth of institutions and
associated knowledge systems that observed and categorized human beings;
among these, the ones significant to the development of today's
concepts of disability were asylums, clinics, and, prisons.
Contemporary concepts of disability are rooted in eighteenth- and
nineteenth-century developments. Foremost among these was the
development of clinical medical discourse, which made the human body
visible as a thing to be manipulated, studied, and transformed. These
worked in tandem with scientific discourses that sought to classify and
categorize and, in so doing, became methods of normalization.
The concept of the "norm" developed in this time period, and is signaled in the work of the Belgianstatistician, sociologist, mathematician, and astronomerAdolphe Quetelet,
who wrote in the 1830s of l'homme moyen – the average man. Quetelet
postulated that one could take the sum of all people's attributes in a
given population (such as their height or weight) and find their
average, and that this figure should serve as a norm toward which all
should aspire.
This idea of a statistical norm threads through the rapid take up
of statistics gathering by Britain, United States, and the Western
European states during this time period, and it is tied to the rise of eugenics. Disability, as well as other concepts including: abnormal, non-normal, and normalcy came from this. The circulation of these concepts is evident in the popularity of the freak show, where showmen profited from exhibiting people who deviated from those norms.
With the rise of eugenics in the latter part of the nineteenth
century, such deviations were viewed as dangerous to the health of
entire populations. With disability viewed as part of a person's
biological make-up and thus their genetic inheritance, scientists turned
their attention to notions of weeding such "deviations" out of the gene
pool. Various metrics for assessing a person's genetic fitness, which
were then used to deport, sterilize, or institutionalize those deemed
unfit. At the end of the Second World War, with the example of Nazi
eugenics, eugenics faded from public discourse, and increasingly
disability cohered into a set of attributes that medicine could attend
to – whether through augmentation, rehabilitation, or treatment. In both
contemporary and modern history, disability was often viewed as a
by-product of incest between first-degree relatives or second-degree relatives.
In the early 1970s, disability activists began to challenge how
society treated disabled people and the medical approach to disability.
Due to this work, physical barriers to access were identified. These conditions functionally disabled them, and what is now known as the social model of disability emerged. Coined by Mike Oliver in 1983, this phrase distinguishes between the medical model of disability
– under which an impairment needs to be fixed – and the social model of
disability – under which the society that limits a person needs to be
fixed.
People-first language is one way to talk about disability that some people prefer. Many others prefer identity-first language.
Using people-first language is said to put the person before the
disability, so those individuals who prefer people-first language,
prefer to be called, "a person with a disability". This style is
reflected in major legislation on disability rights, including the Americans with Disabilities Act and the UN Convention on the Rights of Persons with Disabilities.
For people-first guidelines, check out, "Cerebral Palsy: A Guide for Care" at the University of Delaware:
"The American Psychological Associationstyle guide
states that, when identifying a person with a disability, the person's
name or pronoun should come first, and descriptions of the disability
should be used so that the disability is identified, but is not
modifying the person. Acceptable examples included "a woman with Down syndrome" or "a man who has schizophrenia".
It also states that a person's adaptive equipment should be described
functionally as something that assists a person, not as something that
limits a person, for example, "a woman who uses a wheelchair" rather
than "a woman in/confined to a wheelchair".
A similar
kind of "people-first" terminology is also used in the UK, but more
often in the form "people with impairments" (such as "people with visual
impairments"). However, in the UK, identity-first language is generally
preferred over people-first language.
The use of “people-first” terminology has given rise to the use
of the acronym PWD to refer to person(s) (or people) with disabilities
(or disability).
However other individuals and groups prefer identity-first language to
emphasize how a disability can impact people's identities. Which style
of language used varies between different countries, groups and
individuals.
Identity-first language
In
contrast to people-first language, identity-first language describes
the person as "disabled". Some people prefer this and argue that this
fits the social model even better than does people-first language, as it
emphasizes that the person is disabled not by their body, but by a
world that does not accommodate them.
This is especially true in the UK, where it is argued under the social model
that while someone's impairment (for example, having a spinal cord
injury) is an individual property, "disability" is something created by
external societal factors such as a lack of accessibility. This distinction between the individual property of impairment and the social property of disability is central to the social model.
The term "disabled people" as a political construction is also widely
used by international organisations of disabled people, such as Disabled Peoples' International (DPI).
Using identity-first language also parallels how people talk about other aspects of identity and diversity. For example:
“In
the autism community, many self-advocates and their allies prefer
terminology such as ‘Autistic,’ ‘Autistic person,’ or ‘Autistic
individual’ because we understand autism as an inherent part of an
individual’s identity — the same way one refers to ‘Muslims,’
‘African-Americans,’ ‘Lesbian/Gay/Bisexual/Transgender/Queer,’
‘Chinese,’ ‘gifted,’ ‘athletic,’ or ‘Jewish.’”
Similarly, the Deaf community rejects people-first language in favor of identity-first language.
Aging
To a
certain degree, physical impairments and changing mental states are
almost ubiquitously experienced by people as they age. Aging populations
are often stigmatized for having a high prevalence of disability. Kathleen Woodward, writing in Key Words for Disability Studies, explains the phenomenon as follows:
Aging is invoked rhetorically – at
times ominously – as a pressing reason why disability should be of
crucial interest to all of us (we are all getting older, we will all be
disabled eventually), thereby inadvertently reinforcing the damaging and
dominant stereotype of aging as solely an experience of decline and
deterioration. But little attention has been given to the imbrication of
aging and disability.
Employment
Studies have illustrated a correlation between disability and poverty.
Notably, jobs offered to disabled people are scarce. In the developed
world there are programs in place that aid intellectually disabled (ID)
people to acquire skills they need in the workforce.
Such programs include sheltered workshops and adult day care programs.
Sheltered programs consist of daytime activities such as, gardening,
manufacturing, and assembling. These activities facilitate
routine-oriented tasks that in turn allow intellectually disabled people
to gain experience before entering the workforce. Similarly, adult day
care programs also include day time activities. However, these
activities are based in an educational environment where intellectually
disabled are able to engage in educational, physical, and communication
based tasks. This educational based environment helps facilitate
communication, memory, and general living skills. In addition, adult day
care programs arrange opportunities for their students to engage in
community activities. Such opportunities are arranged by scheduling
field trips to public places (e.g. Disneyland, Zoo, and Movie Theater).
Despite, both programs providing essential skills for intellectually
disabled prior to entering the workforce researchers have found that
intellectually disabled people prefer to be involved with
community-integrated employment. Community-integrated employment are job opportunities offered to
intellectually disabled people at minimum wage or a higher rate
depending on the position. Community-integrated employment comes in a
variety of occupations ranging from customer service, clerical,
janitorial, hospitality and manufacturing positions. Within their daily
tasks community-integrated employees work alongside employees who do not
have disabilities, but who are able to assist them with training. All
three options allow intellectually disabled people to develop and
exercise social skills that are vital to everyday life. However, it is
not guaranteed that community-integrated employees receive the same
treatment as employees that do not have ID. According to Lindstrom,
Hirano, McCarthy, and Alverson, community-integrated employees are less
likely to receive raises. In addition, studies conducted in 2013
illustrated only 26% of employees with ID retained full-time status.
Furthermore, many with disabilities, intellectual and (or)
psychical, finding a stable workforce poses many challenges. According
to a study conducted by JARID (Journal of Applied Research and
Intellectual Disability, indicates that although finding a job may be
difficult for an intellectually disabled individual, stabilizing a job
is even harder.
This is largely due to two main factors: production skills and
effective social skills. This idea is supported by Chadsey-Rusch, who
claims that securing employment for the intellectually disabled,
requires adequate production skills and effective social skills.
However, other underlying factors for job loss include, structural
factors and the integration between worker and workplace. As stated by
Kilsby, limited structural factors can effect a multitude of factors in a
job. Factors such as a restricted number of hours an intellectually
disabled person is allowed to work. This in return, according to Fabian,
Wistow, and Schneider leads to a lack of opportunity to develop
relationships with coworkers and a chance to better integrate within the
workplace. Nevertheless, those who are unable to stabilize a job often
are left discouraged. According to the same study conducted by JARED,
many who had participated, found that they had made smaller incomes when
compared to their co-workers, had an excess of time throughout their
days, because they did not have work. They also had feelings of
hopelessness and failure. According to the NOD ( National Organization
On Disability), not only do the (ID) face constant discouragement, but
many live below the poverty line, because they are unable to find or
stabilize employment and (or) because of employee restricting factors
placed on ID workers.
This then causes the (ID) the incapacity to provide for themselves
basic necessities one needs. Items such as, food, medical care,
transportation, and housing.
There is a global correlation between disability and poverty,
produced by a variety of factors. Disability and poverty may form a
vicious circle, in which physical barriers and stigma of disability make
it more difficult to get income, which in turn diminishes access to
health care and other necessities for a healthy life. The World report on disability indicates that half of all disabled people cannot afford health care, compared to a third of abled people. In countries without public services for adults with disabilities, their families may be impoverished.
Disasters
There is limited research knowledge, but many anecdotal reports, on what happens when disasters impact disabled people. Individuals with disabilities are greatly affected by disasters. Those with physical disabilities can be at risk when evacuating if assistance is not available. Individuals with cognitive impairments may struggle with understanding instructions that must be followed in the event a disaster occurs. All of these factors can increase the degree of variation of risk in disaster situations with disabled individuals.
Research studies have consistently found discrimination against
individuals with disabilities during all phases of a disaster cycle. The most common limitation is that people cannot physically access buildings or transportation, as well as access disaster-related services.
The exclusion of these individuals is caused in part by the lack of
disability-related training provided to emergency planners and disaster relief personnel.
Theory
The International Classification of Functioning, Disability and Health (ICF), produced by the World Health Organization,
distinguishes between body functions (physiological or psychological,
such as vision) and body structures (anatomical parts, such as the eye
and related structures). Impairment in bodily structure or function is
defined as involving an anomaly, defect, loss or other significant
deviation from certain generally accepted population standards, which
may fluctuate over time. Activity is defined as the execution of a task
or action. The ICF lists 9 broad domains of functioning which can be
affected:
Community, social and civic life, including employment
Other major life areas
In concert with disability scholars, the introduction to the ICF
states that a variety of conceptual models have been proposed to
understand and explain disability and functioning, which it seeks to
integrate. These models include the following:
Medical model
The medical model
views disability as a problem of the person, directly caused by
disease, trauma, or other health conditions which therefore requires
sustained medical care in the form of individual treatment by
professionals. In the medical model, management of the disability is
aimed at a "cure", or the individual's adjustment and behavioral change
that would lead to an "almost-cure" or effective cure. In the medical
model, medical care is viewed as the main issue, and at the political
level, the principal response is that of modifying or reforming healthcare policy.
Social model
The social model of disability sees "disability" as a socially created problem and a matter of the full integration of individuals into society.
In this model, disability is not an attribute of an individual, but
rather a complex collection of conditions, created by the social
environment. The management of the problem requires social action
and it is the collective responsibility of society to create a society
in which limitations for disabled people are minimal. Disability is both
cultural and ideological in creation. According to the social model, equal access for someone with an impairment/disability is a human rights concern.
The social model of disability has come under criticism. While
recognizing the importance played by the social model in stressing the
responsibility of society, scholars, including Tom Shakespeare, point out the limits of the model, and urge the need for a new model that will overcome the "medical vs. social" dichotomy.
The limitations of this model mean that often the vital services and
information persons with disabilities face are simply not available,
often due to limited economic returns in supporting them.
Some say medical humanities is a fruitful field where the gap between the medical and the social model of disability might be bridged.
Social construction
The
social construction of disability is the idea that disability is
constructed by social expectations and institutions rather than
biological differences. Highlighting the ways society and institutions
construct disability is one of the main focuses of this idea. In the same way that race and gender are not biologically fixed, neither is disability.
Around the early 1970s, sociologists, notably Eliot Friedson, began to argue that labeling theory and social deviance could be applied to disability studies. This led to the creation of the social construction of disability
theory. The social construction of disability is the idea that
disability is constructed as the social response to a deviance from the
norm. The medical industry is the creator of the ill and disabled social
role. Medical professionals and institutions, who wield expertise over
health, have the ability to define health and physical and mental norms.
When an individual has a feature that creates an impairment,
restriction, or limitation from reaching the social definition of
health, the individual is labeled as disabled. Under this idea,
disability is not defined by the physical features of the body but by a
deviance from the social convention of health.
Social construction of disability would argue that the medical model of disability's
view that a disability is an impairment, restriction, or limitation is
wrong. Instead what is seen as a disability is just a difference in the
individual from what is considered "normal" in society.
Other models
The spectrum model
refers to the range of audibility, sensibility, and visibility under
which people function. The model asserts that disability does not
necessarily mean reduced spectrum of operations. Rather, disability is
often defined according to thresholds set on a continuum of disability.
The moral model refers to the attitude that people are morally responsible for their own disability. For example, disability may be seen as a result of bad actions of parents if congenital, or as a result of practicing witchcraft if not. Echoes of this can be seen in the doctrine of karma
in Indian religions. It also includes notions that a disability gives a
person "special abilities to perceive, reflect, transcend, be
spiritual".
The expert/professional model has provided a traditional
response to disability issues and can be seen as an offshoot of the
medical model. Within its framework, professionals follow a process of
identifying the impairment and its limitations (using the medical
model), and taking the necessary action to improve the position of the
disabled person. This has tended to produce a system in which an
authoritarian, over-active service provider prescribes and acts for a
passive client.
The tragedy/charity model depicts disabled people as victims
of circumstance who are deserving of pity. This, along with the medical
model, are the models most used by non-disabled people to define and
explain disability.
The legitimacy model views disability as a value-based
determination about which explanations for the atypical are legitimate
for membership in the disability category. This viewpoint allows for
multiple explanations and models to be considered as purposive and
viable.
The social adapted model states although a person's
disability poses some limitations in an able-bodied society, often the
surrounding society and environment are more limiting than the
disability itself.
The economic model defines disability in terms of reduced
ability to work, the related loss of productivity and economic effects
on the individual, employer and society in general.
The empowering model (also, customer model) allows for
the person with a disability and his/her family to decide the course of
his/her treatment. This turns the professional into a service provider
whose role is to offer guidance and carry out the client's decisions.
This model "empowers" the individual to pursue his/her own goals.
The market model of disability is minority rights and
consumerist model of disability that recognizing disabled people and
their stakeholders as representing a large group of consumers, employees
and voters. This model looks to personal identity to define disability
and empowers people to chart their own destiny in everyday life, with a
particular focus on economic empowerment. By this model, based on US
Census data, there are 1.2 billion people in the world who consider
themselves to have a disability. "This model states that, due to the
size of the demographic, companies and governments will serve the
desires, pushed by demand as the message becomes prevalent in the
cultural mainstream."
The consumer model of disability is based upon the
“rights-based" model and claims that disabled people should have equal
rights and access to products, goods and services offered by businesses.
The consumer model extends the rights-based model by proposing that
businesses, not only accommodate customers with disabilities under the
requirements of legislation, but that businesses actively seek, market
to, welcome and fully engage disabled people in all aspects of business
service activities. The model suggests that all business operations,
for example websites, policies and procedures, mission statements,
emergency plans, programs and services, should integrate access and
inclusion practices. Furthermore, these access and inclusion practices
should be based on established customer service access and inclusion
standards that embrace and support the active engagement of people of
all abilities in business offerings.
In this regard, specialized products and specialized services become
important, such as auxiliary means, protheses, special foods, domestic
help, and assisted living.
Different theories revolve around prejudice, stereotyping,
discrimination, and stigma related to disability. One of the more
popular ones, as put by Weiner, Perry, and Magnusson 's (1988) work with
attribution theory, physical stigmas are perceived as to be
un-controllable and elicit pity and desire to help, whereas,
mental-behavioral stigmas are considered to be controllable and
therefore elicit anger and desire to neglect the individuals with
disabilities.
The ‘just world hypothesis’ talks about how a person is
viewed as deserving the disability. And because it is the fault of that
person, an observer does not feel obligated to feel bad for him or to
help him.
Identity
In
contexts where their differences are visible, persons with disabilities
often face stigma. People frequently react to disabled presence with
fear, pity, patronization, intrusive gazes, revulsion, or disregard.
These reactions can, and often do, exclude persons with disabilities
from accessing social spaces along with the benefits and resources these
spaces provide. Disabled writer/researcher Jenny Morris describes how stigma functions to marginalize persons with disabilities:
“Going out in public so often takes
courage. How many of us find that we can't dredge up the strength to do
it day after day, week after week, year after year, a lifetime of
rejection and revulsion? It is not only physical limitations that
restrict us to our homes and those whom we know. It is the knowledge
that each entry into the public world will be dominated by stares, by
condescension, by pity and by hostility.”
Additionally, facing stigma can cause harm to psycho-emotional
well-being of the person being stigmatized. One of the ways in which the
psycho-emotional health of persons with disabilities is adversely
affected is through the internalization of the oppression they
experience, which can lead to feeling that they are weak, crazy,
worthless, or any number of other negative attributes that may be
associated with their conditions. Internalization of oppression damages
the self-esteem of the person affected and shapes their behaviors in
ways that are compliant with nondisabled dominance.
Ableist ideas are frequently internalized when disabled people are
pressured by the people and institutions around them to hide and
downplay their disabled difference, or, "pass". According to writer Simi
Linton, the act of passing takes a deep emotional toll by causing
disabled individuals to experience loss of community, anxiety and
self-doubt.
The media play a significant role in creating and reinforcing stigma
associated with disability. Media portrayals of disability usually cast
disabled presence as necessarily marginal within society at large. These
portrayals simultaneously reflect and influence the popular perception
of disabled difference.
Tropes
There are distinct tactics that the media frequently employ in
representing disabled presence. These common ways of framing disability
are heavily criticized for being dehumanizing and failing to place
importance on the perspectives of persons with disabilities.
Inspiration porn
Inspiration porn
refers to portrayals of persons with disabilities in which they are
presented as being inspiring simply because the person has a disability.
These portrayals are criticized because they are created with the
intent of making non-disabled viewers feel better about themselves in
comparison to the individual portrayed. Rather than recognizing the
humanity of persons with disabilities, inspiration porn turns them into
objects of inspiration for a non-disabled audience.
Supercrip
The
supercrip trope refers to instances when media reports on or portray a
disabled person who has made a noteworthy achievement; but center on
their disability rather than what they actually did. They are portrayed
as awe-inspiring for being exceptional compared to others with the same
or similar conditions. This trope is widely used in reporting on
disabled athletes as well as in portrayals of autistic savants.
Many disabled people denounce these representations as reducing
people to their condition rather than viewing them as full people.
Furthermore, supercrip portrayals are criticized for creating the
unrealistic expectation that disability should be accompanied by some
type of special talent, genius, or insight.
Disabled villain
Characters
in fiction that bear physical or mental markers of difference from
perceived societal norms are frequently positioned as villains within a
text. Lindsey Row-Heyveld notes, for instance, “that villainous pirates
are scraggly, wizened, and inevitably kitted out with a peg leg, eye
patch, or hook hand whereas heroic pirates look like Johnny Depp's Jack Sparrow.”
Disabled people's visible differences from the abled majority are
meant to evoke fear in audiences that can perpetuate the mindset of
disabled people being a threat to individual or public interests and
well-being.
Self advocacy
Some disabled people have attempted to resist marginalisation
through the use of the social model in opposition to the medical model;
with the aim of shifting criticism away from their bodies and
impairments and towards the social institutions that oppress them
relative to their abled peers. Disability activism that demands many
grievances be addressed, such as lack of accessibility, poor representation in media, general disrespect, and lack of recognition, originates from a social model framework.
Embracing disability as a positive identity by becoming involved
in disabled communities and participating in disabled culture can be an
effective way to combat internalised prejudice; and can challenge
dominant narratives about disability.
Intersections
The experiences that disabled people have navigating social
institutions vary greatly as a function of what other social categories
they may belong to. The categories that intersect with disability to
create unique experiences of ableism include, but aren't limited to,
race and gender. The United Nations Convention on the Rights of Persons
with Disabilities differentiates two kinds of disability intersection,
race disability intersection and gender disability intersection.
Race
Disabled people who are also racial minorities
generally have less access to support and are more vulnerable to
violent discrimination. For example, in the United States people of
color who are mentally ill are more frequently victims of police
brutality than their white counterparts. Camille A. Nelson, writing for
the Berkeley Journal of Criminal Law, notes that for “people who
are negatively racialized, that is people who are perceived as being
non-white, and for whom mental illness is either known or assumed,
interaction with police is precarious and potentially dangerous.”
Gender
The
marginalization of disabled people can leave persons with disabilities
unable to actualize what society expects of gendered existence. This
lack of recognition for their gender identity can leave persons with
disabilities with feelings of inadequacy. Thomas J. Gerschick of
Illinois State University describes why this denial of gendered identity
occurs:
Bodies operate socially as canvases
on which gender is displayed and kinesthetically as the mechanisms by
which it is physically enacted. Thus, the bodies of disabled people make
them vulnerable to being denied recognition as women and men.
To the extent that women and men with disabilities are gendered, the
interactions of these two identities lead to different experiences.
Disabled women face a sort of “double stigmatization”
in which their membership to both of these marginalized categories
simultaneously exacerbates the negative stereotypes associated with each
as they are ascribed to them. According to The UN Woman Watch,
"Persistence of certain cultural, legal and institutional barriers makes
women and girls with disabilities the victims of two-fold
discrimination: as women and as persons with disabilities."
As Rosemarie Garland-Thomson puts it, “Women with disabilities, even
more intensely than women in general, have been cast in the collective
cultural imagination as inferior, lacking, excessive, incapable, unfit,
and useless.”
As the personal computer has become more ubiquitous, various organizations have formed to develop software and hardware to make computers more accessible for disabled people. Some software and hardware, such as Voice Finger, Freedom Scientific's JAWS, the Free and Open Source alternative Orca etc. have been specifically designed for disabled people while other software and hardware, such as Nuance's Dragon NaturallySpeaking, were not developed specifically for disabled people, but can be used to increase accessibility. The LOMAK keyboard was designed in New Zealand specifically for persons with disabilities.
The World Wide Web consortium recognised a need for International
Standards for Web Accessibility for persons with disabilities and
created the Web Accessibility Initiative (WAI). As at Dec 2012 the standard is WCAG 2.0 (WCAG = Web Content Accessibility Guidelines).
The Paralympic Games (meaning "alongside the Olympics") are held after the (Summer and Winter) Olympics.
The Paralympic Games include athletes with a wide range of physical
disabilities. In member countries, organizations exist to organize
competition in the Paralympic sports on levels ranging from recreational
to elite (for example, Disabled Sports USA and BlazeSports America in the United States).
The Paralympics developed from a rehabilitation programme for
British war veterans with spinal injuries. In 1948, Sir Ludwig Guttman, a
neurologist working with World War II veterans with spinal injuries at Stoke Mandeville Hospital in Aylesbury in the UK, began using sport as part of the rehabilitation programmes of his patients.
In 2006, the Extremity Games were formed for physically disabled people, specifically limb loss or limb difference, to be able to compete in extreme sports.
Rights and government policies
Rights movement
The disability rights movement aims to secure equal opportunities and
equal rights for disabled people. The specific goals and demands of the
movement are accessibility and safety
in transportation, architecture, and the physical environment; equal
opportunities in independent living, employment, education, and housing;
and freedom from abuse, neglect, and violations of patients' rights. Effective civil rights legislation is sought to secure these opportunities and rights.
The early disability rights movement was dominated by the medical
model of disability, where emphasis was placed on curing or treating
disabled people so that they would adhere to the social norm, but
starting in the 1960s, rights groups began shifting to the social model
of disability, where disability is interpreted as an issue of
discrimination, thereby paving the way for rights groups to achieve
equality through legal means.
Policies and actions
Convention on the Rights of Persons with Disabilities
On December 13, 2006, the United Nations formally agreed on the Convention on the Rights of Persons with Disabilities,
the first human rights treaty of the 21st century, to protect and
enhance the rights and opportunities of the world's estimated 650
million disabled people. As of April 2011, 99 of the 147 signatories had ratified the Convention.
Countries that sign the convention are required to adopt national laws,
and remove old ones, so that persons with disabilities will, for
example, have equal rights to education, employment, and cultural life;
to the right to own and inherit property; to not be discriminated
against in marriage, etc.; and to not be unwilling subjects in medical
experiments. UN officials, including the High Commissioner for Human
Rights, have characterized the bill as representing a paradigm shift in
attitudes toward a more rights-based view of disability in line with the
social model.
International Year of Disabled Persons
In 1976, the United Nations began planning for its International Year of Disabled Persons (1981), later renamed the International Year of Disabled Persons. The UN Decade of Disabled Persons (1983–1993) featured a World Programme of Action Concerning Disabled Persons. In 1979, Frank Bowe
was the only person with a disability representing any country in the
planning of IYDP-1981. Today, many countries have named representatives
who are themselves individuals with disabilities. The decade was closed
in an address before the General Assembly by Robert Davila. Both Bowe and Davila are deaf. In 1984, UNESCO accepted sign language for use in education of deaf children and youth.
Policies in the United States
In
the United States, the Department of Labor's 2014 rules for federal
contractors, defined as companies that make more than $50,000/year from
the federal government, required them to have as a goal that 7% of their
workforce must be disabled people. In schools, the ADA says that all classrooms must be wheelchair accessible.
The U.S. Architectural and Transportation Barriers Compliance Board,
commonly known as the Access Board, created the Rehabilitation Act of
1973 to help offer guidelines for transportation and accessibility for
the physically disabled.
About 12.6% of the U.S. population are individuals who suffer
from a mental or physical disability. Many are unemployed because of
prejudiced assumptions that a person with disabilities is unable to
complete tasks that are commonly required in the workforce. This became a
major Human rights
issue because of the discrimination that this group faced when trying
to apply for jobs in the U.S. Many advocacy groups protested against
such discrimination, asking the federal government to implement laws and policies that would help individuals with disabilities.
Rehabilitation Act of 1973
The Rehabilitation Act of 1973
was enacted with the purpose of protecting individuals with
disabilities from prejudicial treatment by government funded programs,
employers, and agencies. The Rehabilitation Act of 1973 has not only
helped protect U.S. citizens from being discriminated against but it has
also created confidence amongst individuals to feel more comfortable
with their disability. There are many sections within The Rehabilitation
Act of 1973, that contains detailed information about what is covered
in this policy.
Section 501
An employer must hire an individual who meets the qualifications of a job description despite any preexisting disabilities.
Section 503
Requires contractors or subcontractors, who receive more than
$10,000 from the government to hire people with disabilities and to
accommodate them with the needs that they need to achieve in the work
force.
States that receive federal money may not discriminate against any person with disabilities who qualifies for a program or job.
On June 22, 1999 the United States Supreme Court issued a ruling in
Olmstead vs. L. C. that said unjustified segregation of persons with
disabilities constitutes discrimination in violation of title II of the
Americans with Disabilities Act. This has been interpreted as meaning
people with disabilities must be given all opportunity by government to
stay in their own homes as opposed to assisted living, nursing homes or
worse, institutions for the disabled. It's been interpreted as meaning
government must make all reasonable efforts to allow people with
disabilities to be included in their respective communities and enjoy
family and friends, work if possible, get married, own homes and
interact with nondisabled people. This is why the United States has so
many community based services today for the disabled including but not
limited to home health aides, personal care attendants and other
programs to keep people with disabilities in their own homes and
communities.
The Americans with Disabilities Act of 1990
The
federal government enacted The Americans with Disabilities Act of 1990,
which was created to allow equal opportunity for jobs, access to
private and government funded facilities, and transportation for
disabled people. This act was created with the purpose to ensure that
employers would not discriminate against any individual despite their
disability. In 1990, data was gathered to show the percentage of
disabled people who worked in the U.S. Out of the 13% who filled out the
survey, only 53% percent of individuals with disabilities worked while
90% of this group population did not, the government wanted to change
this, they wanted Americans with disabilities to have the same
opportunities as those who did not have a disability. The ADA not only required corporations to hire disabled people but that they also accommodate them and their needs.
Title I
Employment
An employer must give a qualified individual with disabilities the
same opportunities as any other employee despite their disability. The
employer must offer equal work privileges to someone who has a
disability including but not limited to pay, work hours, training, etc.
The employer must also create accommodations suitable for the person and
their physical or mental disabilities.
Title II
State and Local Government Activities
Requires that the government give disabled people the same
opportunities involving work, programs, building access, and services.
Title II also requires that buildings create easy access for disabled
people and provide communicators who will be able to help those with hearing
or speaking impairments. Public spaces are however not required to
create accommodations that would in turn alter their services as long as
the services proved that they did all they could to prevent
discrimination against disabled people.
Title II
Transportation
Public transportation should be customized so that disabled people may have easy access to public transit. Paratransit
is a service that provides transportation to people who are unable to
get from one destination to another due to their mental or physical
disability.
Title II
Public Accommodations
Public accommodations require that private businesses create
accommodations that will allow disabled people easy access to buildings.
Private businesses may not discriminate against disabled people and
must provide accommodations that are reasonable, alterations may be made
so that a person with disabilities can have equal access to facilities
that are provided, communicators for the hearing impaired, devices for the visually impaired, and wheelchair access. Facilities must regulate with the ADA, when regulating the buildings infrastructure so it meets the ADA regulations.
Title IV
Telecommunication Relay Services
Requires telephone companies to have TRS
seven days a week, twenty four hours a day. It requires telephone
companies to create accommodations for deaf/hard of hearing people by
providing a third party that will be able to assistant both parties in
communicating with one another.
Policies in the United Kingdom
In
the UK, the Department for Work and Pension is a government department
responsible for promoting disability awareness and among its aims is to
increase the understanding of disability and removal of barriers for
disabled people in the workplace. According to a news report, a people
survey conducted in the UK shows a 23% increase in reported
discrimination and harassment in the workplace at The Department for
Work and Pension. The survey shows the number of reports for
discrimination due to disability was in majority compared to
discrimination due to gender, ethnicity or age. DWP received criticism
for the survey results. As a department responsible for tackling
discrimination at work, the DWP results may indicate room for
improvement from within. A DWP spokesperson said the survey results do
not necessarily indicate an increase in the number of reports, but
rather reflecting the outcomes of efforts to encourage people to come
forward.
Political issues
A 28-year-old Iraqi woman who lost both of her legs during the Iraq War in 2005
Political rights, social inclusion and citizenship
have come to the fore in developed and some developing countries. The
debate has moved beyond a concern about the perceived cost of
maintaining dependent disabled people to finding effective ways to
ensure that disabled people can participate in and contribute to society
in all spheres of life.
In developing nations, where the vast bulk of the estimated 650
million disabled people reside, a great deal of work is needed to
address concerns ranging from accessibility and education to
self-empowerment, self-supporting employment, and beyond.
In the past few years, disability rights activists have focused on obtaining full citizenship for the disabled.
There are obstacles in some countries in getting full employment; public perception of disabled people may vary.
Abuse
Disability abuse happens when a person is abused physically,
financially, verbally or mentally due to the person having a disability.
As many disabilities are not visible (for example, asthma, learning
disabilities) some abusers cannot rationalize the non-physical
disability with a need for understanding, support, and so on.
As the prevalence of disability and the cost of supporting
disability increases with medical advancement and longevity in general,
this aspect of society becomes of greater political importance. How
political parties treat their disabled constituents may become a measure
of a political party's understanding of disability, particularly in the
social model of disability.
Insurance
Disability benefit, or disability pension, is a major kind of disability insurance
that is provided by government agencies to people who are temporarily
or permanently unable to work due to a disability. In the U.S.,
disability benefit is provided in the category of Supplemental Security Income. In Canada, it is within the Canada Pension Plan. In other countries, disability benefit may be provided under social security systems.
Costs of disability pensions are steadily growing in Western
countries, mainly in Europe and the United States. It was reported that,
in the UK, expenditure on disability pensions accounted for 0.9% of
gross domestic product (GDP) in 1980; two decades later it had reached
2.6% of GDP.[91][93]
Several studies have reported a link between increased absence from
work due to sickness and elevated risk of future disability pension.
A study by researchers in Denmark suggests that information on
self-reported days of absence due to sickness can be used to effectively
identify future potential groups for disability pension. These studies may provide useful information for policy makers, case managing authorities, employers, and physicians.
In Switzerland, social policies in the field of disability have
been significantly reshaped over the last two decades by reducing the
number of allowances awarded and by increasing the recourse to
vocational rehabilitation measures. Drawing on interviews conducted with
individuals who have been involved in programmes set up by Swiss
disability insurance, a study highlights their uncertainties and
concerns relating to their place in society, as well as their reactions
to disability insurance's interventions.
Private, for-profit disability insurance plays a role in
providing incomes to disabled people, but the nationalized programs are
the safety net that catch most claimants.
Demographics
Estimates
of worldwide and country-wide numbers of individuals with disabilities
are problematic. The varying approaches taken to defining disability
notwithstanding, demographers agree that the world population of
individuals with disabilities is very large. For example, in 2012, the World Health Organization
estimated a world population of 6.5 billion people. Of those, nearly
650 million people, or 10%, were estimated to be moderately or severely
disabled. In 2018 the International Labour Organization
estimated that about a billion people, one seventh of the world
population, had disabilities, 80% of them in developing countries, and
80% of working age. Excluding disabled people from the workforce was
reckoned to cost up to 7% of gross domestic product.
Afghanistan
After years of war in Afghanistan, there are more than 1 million disabled people. Afghanistan has one of the highest incidences of disabled people in the world. An estimated 80,000 Afghans are missing limbs, usually from landmine explosions.
Australia
More than 4 million people in Australia
have some form of disability as of 2018. Approximately 18.6% of females
and 18.0% of males are said to be affected. 50.7% of Australians aged
65 and over have disability, as opposed to 12.5% aged under 65.
United States
According to the U.S. Census Bureau, as of 2010,
there were some 56.7 million disabled people, or 19% (by comparison,
African Americans are the largest racial minority in the U.S., but only
constitute 12.6% of the U.S. population).
Disabled individuals make up one of the most inclusive minority groups in the United States.
According to the 2014 Disability status report of the Cornell
University Yang Tan Institute the prevalence rate of individuals with
disabilities in the United States was 12.6% in that year. As of 2014
ambulatory disability had the highest prevalence (7.1%) in the United
States. By contrast, visual disability had the lowest prevalence (2.3%).
Additionally, 3.6% of people in the United States were reported to have
had an auditory disability in the same year.
5.8% of individuals ages 16–20 reported having any disability,
physical and/ or cognitive. Adults 21 to 64 had a prevalence of 10.8%
with over half of these (5.5%) being ambulatory disabilities. Ambulatory
disability prevalence raised to 15.8% in adults 65–74 years of age.
Adults 75 years and older comprised the highest prevalence with any
disability at 50.3%.
Female individuals across all ages reported a total 0.4% higher prevalence rate than males who reported 12.4%.
In the U.S. 17.9% of Native American peoples reported having a
disability while 4.5% reporting were of Asian descent, these were the
two opposing poles of the prevalence rate within race as of 2014.
Although there are acts that have been imposed in order to
prevent the discrimination of individuals with disabilities in the
workplace, there is still an employment gap that can be seen between
those with and without disabilities. In regards to employment, the
institute's status report accounts that 34.6% of people with any
disability reported being employed. By comparison; 77.6% of individuals,
who did not report having a disability, reported having a full-time job
in 2014.
For those employed full-time, individuals with disabilities on
average earned $5,100 less than employees without a disability who were
also employed full-time. Those affected the most by these differences
were intellectually disabled people. As of 2008, there were 2.9 million disabled veterans in the United States, an increase of 25 percent over 2001.
Europe
Nearly 8 million European men were permanently disabled in World War I. About 150,000 Vietnam veterans came home wounded, and at least 21,000 were permanently disabled.
Developing nations
There is widespread agreement among experts in the field, that disability is more common in developing than in developed nations. The connection between disability and poverty is thought to be part of a "vicious cycle" in which these constructs are mutually reinforcing.