 | |
| Abbreviation | IPCC |
|---|---|
| Formation | 1988 |
| Type | Panel |
| Legal status | Active |
| Headquarters | Geneva, Switzerland |
Head
| Hoesung Lee |
Parent organization
| World Meteorological Organization United Nations Environment Program |
| Website | ipcc |
The Intergovernmental Panel on Climate Change (IPCC) is an intergovernmental body of the United Nations that is dedicated to providing the world with an objective, scientific view of climate change, its natural, political, and economic impacts and risks, and possible response options.
The IPCC was established in 1988 by the World Meteorological Organization (WMO) and the United Nations Environment Programme (UNEP) and was later endorsed by the United Nations General Assembly. Membership is open to all members of the WMO and UN. The IPCC produces reports that contribute to the work of the United Nations Framework Convention on Climate Change (UNFCCC), the main international treaty on climate change. The objective of the UNFCCC is to "stabilize greenhouse gas concentrations in the atmosphere at a level that would prevent dangerous anthropogenic (human-induced) interference with the climate system". The IPCC's Fifth Assessment Report was a critical scientific input into the UNFCCC's Paris Agreement in 2015.
IPCC reports cover the "scientific, technical and socio-economic information relevant to understanding the scientific basis of risk of human-induced climate change, its potential impacts and options for adaptation and mitigation." The IPCC does not carry out original research, nor does it monitor climate or related phenomena itself. Rather, it assesses published literature, including peer-reviewed and non-peer-reviewed sources. However, the IPCC can be said to stimulate research in climate science. Chapters of IPCC reports often close with sections on limitations and knowledge or research gaps, and the announcement of an IPCC special report can catalyse research activity in that area.
Thousands of scientists and other experts contribute on a voluntary basis to writing and reviewing reports, which are then reviewed by governments. IPCC reports contain a "Summary for Policymakers", which is subject to line-by-line approval by delegates from all participating governments. Typically, this involves the governments of more than 120 countries.
The IPCC provides an internationally accepted authority on climate change, producing reports that have the agreement of leading climate scientists and consensus from participating governments. The 2007 Nobel Peace Prize was shared between the IPCC and Al Gore.
Following the election of a new Bureau in 2015, the IPCC embarked on its sixth assessment cycle. Besides the Sixth Assessment Report, to be completed in 2022, the IPCC released the Special Report on Global Warming of 1.5 °C in October 2018, released an update to its 2006 Guidelines for National Greenhouse Gas Inventories—the 2019 Refinement—in May 2019, and delivered two further special reports in 2019: the Special Report on Climate Change and Land (SRCCL), published online on August 7, and the Special Report on the Ocean and Cryosphere in a Changing Climate (SROCC), released on September 25, 2019. This makes the sixth assessment cycle the most ambitious in the IPCC's 30-year history. The IPCC also decided to prepare a special report on cities and climate change in the seventh assessment cycle and held a conference in March 2018 to stimulate research in this area.
Origins and aims
The IPCC developed from an international scientific body, the Advisory Group on Greenhouse Gases set up in 1985 by the International Council of Scientific Unions, the United Nations Environment Programme (UNEP), and the World Meteorological Organization
(WMO) to provide recommendations based on current research. This small
group of scientists lacked the resources to cover the increasingly
complex interdisciplinary nature of climate science. The United States Environmental Protection Agency and State Department wanted an international convention to agree restrictions on greenhouse gases, and the conservative Reagan Administration
was concerned about unrestrained influence from independent scientists
or from United Nations bodies including UNEP and the WMO. The U.S.
government was the main force in forming the IPCC as an autonomous
intergovernmental body in which scientists took part both as experts on
the science and as official representatives of their governments, to
produce reports which had the firm backing of all the leading scientists
worldwide researching the topic, and which then had to gain consensus
agreement from every one of the participating governments. In this way,
it was formed as a hybrid between a scientific body and an
intergovernmental political organisation.
The United Nations formally edorsed the creation of the IPCC in
1988. Some of the reasons the UN stated in its resolution include
- "[C]ertain human activities could change global climate patterns, threatening present and future generations with potentially severe economic and social consequences"
- "[C]ontinued growth in atmospheric concentrations of "greenhouse" gases could produce global warming with an eventual rise in sea levels, the effects of which could be disastrous for mankind if timely steps are not taken at all levels."
The IPCC was tasked with reviewing peer-reviewed scientific
literature and other relevant publications to provide information on the
state of knowledge about climate change.
Organization
The
IPCC does not conduct its own original research. It produces
comprehensive assessments, reports on special topics, and methodologies.
The assessments build on previous reports, highlighting the latest
knowledge. For example, the wording of the reports from the first to the
fifth assessment reflects the growing evidence for a changing climate
caused by human activity.
The IPCC has adopted and published "Principles Governing IPCC Work", which states that the IPCC will assess:
- the risk of human-induced climate change,
- its potential impacts, and
- possible options for prevention.
This document also states that IPCC will do this work by assessing
"on a comprehensive, objective, open and transparent basis the
scientific, technical and socio-economic information relevant to
understanding the scientific basis" of these topics. The Principles also
state that "IPCC reports should be neutral with respect to policy,
although they may need to deal objectively with scientific, technical
and socio-economic factors relevant to the application of particular
policies."
Korean economist Hoesung Lee has been the chair of the IPCC since 8 October 2015, with the election of the new IPCC Bureau.
Before this election, the IPCC was led by Vice-Chair Ismail El Gizouli, who was designated acting Chair after the resignation of Rajendra K. Pachauri in February 2015. The previous chairs were Rajendra K. Pachauri, elected in May 2002; Robert Watson in 1997; and Bert Bolin in 1988. The chair is assisted by an elected bureau including vice-chairs and working group co-chairs, and by a secretariat.
The Panel itself is composed of representatives appointed by
governments. Participation of delegates with appropriate expertise is
encouraged. Plenary sessions of the IPCC and IPCC Working Groups are held at the level of government representatives. Non-Governmental and Intergovernmental Organizations admitted as observer organizations may also attend. Sessions of the Panel, IPCC Bureau, workshops, expert and lead authors meetings are by invitation only.
About 500 people from 130 countries attended the 48th Session of the
Panel in Incheon, Republic of Korea, in October 2018, including 290
government officials and 60 representatives of observer organizations.
The opening ceremonies of sessions of the Panel and of Lead Author
Meetings are open to media, but otherwise IPCC meetings are closed.
There are several major groups:
- IPCC Panel: Meets in plenary session about once a year. It controls the organization's structure, procedures, and work programme, and accepts and approves IPCC reports. The Panel is the IPCC corporate entity.
- Chair: Elected by the Panel.
- Secretariat: Oversees and manages all activities. Supported by UNEP and WMO.
- Bureau: Elected by the Panel. Chaired by the Chair. 34 members include IPCC Vice-Chairs, Co-Chairs of Working Groups and the Task Force, and Vice-Chairs of the Working Groups. It provides guidance to the Panel on the scientific and technical aspects of its work.
- Working Groups: Each has two Co-Chairs, one from the developed and
one from developing world, and a technical support unit. Sessions of the
Working Group approve the Summary for Policymakers of special reports
and working group contributions to an assessment report. Each Working
Group has a Bureau comprising its Co-Chairs and Vice-Chairs, who are
also members of the IPCC Bureau.
- Working Group I: Assesses scientific aspects of the climate system and climate change. Co-Chairs: Valérie Masson-Delmotte and Panmao Zhai
- Working Group II: Assesses vulnerability of socio-economic and natural systems to climate change, consequences, and adaptation options. Co-Chairs: Hans-Otto Pörtner and Debra Roberts
- Working Group III: Assesses options for limiting greenhouse gas emissions and otherwise mitigating climate change. Co-Chairs: Priyadarshi R. Shukla and Jim Skea
- Task Force on National Greenhouse Gas Inventories. Co-Chairs: Kiyoto Tanabe and Eduardo Calvo Buendía
- Task Force Bureau: Comprises the two Co-Chairs, who are also members of the IPCC Bureau, and 12 members.
- Executive Committee: Comprises the Chair, IPCC Vice-Chairs and the Co-Chairs of the Working Groups and Task Force. Its role includes addressing urgent issues that arise between sessions of the Panel.
The IPCC receives funding through the IPCC Trust Fund, established in 1989 by the United Nations Environment Programme (UNEP) and the World Meteorological Organization
(WMO), Costs of the Secretary and of housing the secretariat are
provided by the WMO, while UNEP meets the cost of the Depute Secretary.
Annual cash contributions to the Trust Fund are made by the WMO, by
UNEP, and by IPCC Members. Payments and their size are voluntary. The
Panel is responsible for considering and adopting by consensus the
annual budget. The organization is required to comply with the Financial
Regulations and Rules of the WMO.
Assessment reports
The IPCC has published five comprehensive assessment reports reviewing the latest climate science,
as well as a number of special reports on particular topics. These
reports are prepared by teams of relevant researchers selected by the
Bureau from government nominations. Expert reviewers from a wide range
of governments, IPCC observer organizations and other organizations are
invited at different
stages to comment on various aspects of the drafts.
The IPCC published its First Assessment Report (FAR) in 1990, a supplementary report in 1992, a Second Assessment Report (SAR) in 1995, a Third Assessment Report (TAR) in 2001, a Fourth Assessment Report (AR4) in 2007 and a Fifth Assessment Report (AR5) in 2014. The IPCC is currently preparing the Sixth Assessment Report (AR6), which will be completed in 2022.
Each assessment report is in three volumes, corresponding to
Working Groups I, II, and III. It is completed by a synthesis report
that integrates the working group contributions and any special reports
produced in that assessment cycle.
Scope and preparation of the reports
The
IPCC does not carry out research nor does it monitor climate related
data. Lead authors of IPCC reports assess the available information
about climate change based on published sources. According to IPCC guidelines, authors should give priority to peer-reviewed sources. Authors may refer to non-peer-reviewed sources (the "grey literature"), provided that they are of sufficient quality.
Examples of non-peer-reviewed sources include model results, reports
from government agencies and non-governmental organizations, and
industry journals.
Each subsequent IPCC report notes areas where the science has improved
since the previous report and also notes areas where further research is
required.
There are generally three stages in the review process:
- Expert review (6–8 weeks)
- Government/expert review
- Government review of:
- Summaries for Policymakers
- Overview Chapters
- Synthesis Report
Review comments are in an open archive for at least five years.
There are several types of endorsement which documents receive:
- Approval. Material has been subjected to detailed, line by line discussion and agreement.
- Working Group Summaries for Policymakers are approved by their Working Groups.
- Synthesis Report Summary for Policymakers is approved by Panel.
- Adoption. Endorsed section by section (and not line by line).
- Panel adopts Overview Chapters of Methodology Reports.
- Panel adopts IPCC Synthesis Report.
- Acceptance. Not been subject to line by line discussion and
agreement, but presents a comprehensive, objective, and balanced view of
the subject matter.
- Working Groups accept their reports.
- Task Force Reports are accepted by the Panel.
- Working Group Summaries for Policymakers are accepted by the Panel after group approval.
The Panel is responsible for the IPCC and its endorsement of Reports allows it to ensure they meet IPCC standards.
There have been a range of commentaries on the IPCC's procedures,
examples of which are discussed later in the article (see also IPCC Summary for Policymakers). Some of these comments have been supportive, while others have been critical. Some commentators have suggested changes to the IPCC's procedures.
Authors
Each chapter has a number of authors who are responsible for writing
and editing the material. A chapter typically has two "coordinating lead
authors", ten to fifteen "lead authors", and a somewhat larger number
of "contributing authors". The coordinating lead authors are responsible
for assembling the contributions of the other authors, ensuring that
they meet stylistic and formatting requirements, and reporting to the
Working Group chairs. Lead authors are responsible for writing sections
of chapters. Contributing authors prepare text, graphs or data for
inclusion by the lead authors.
Authors for the IPCC reports are chosen from a list of
researchers prepared by governments and participating organisations, and
by the Working Group/Task Force Bureaux, as well as other experts known
through their published work. The choice of authors aims for a range of
views, expertise and geographical representation, ensuring
representation of experts from developing and developed countries and
countries with economies in transition.
First assessment report
The IPCC First Assessment Report (FAR) was completed in 1990, and served as the basis of the UNFCCC.
The executive summary of the WG I Summary for Policymakers report
says they are certain that emissions resulting from human activities
are substantially increasing the atmospheric concentrations of the greenhouse gases, resulting on average in an additional warming of the Earth's surface. They calculate with confidence that CO2
has been responsible for over half the enhanced greenhouse effect. They
predict that under a "business as usual" (BAU) scenario, global mean
temperature will increase by about 0.3 °C per decade during the [21st]
century. They judge that global mean surface air temperature has
increased by 0.3 to 0.6 °C over the last 100 years, broadly consistent
with prediction of climate models, but also of the same magnitude as
natural climate variability. The unequivocal detection of the enhanced
greenhouse effect is not likely for a decade or more.
Supplementary report of 1992
The 1992 supplementary report was an update, requested in the context of the negotiations on the UNFCCC at the Earth Summit (United Nations Conference on Environment and Development) in Rio de Janeiro in 1992.
The major conclusion was that research since 1990 did "not affect
our fundamental understanding of the science of the greenhouse effect
and either confirm or do not justify alteration of the major conclusions
of the first IPCC scientific assessment". It noted that transient
(time-dependent) simulations, which had been very preliminary in the
FAR, were now improved, but did not include aerosol or ozone changes.
Second assessment report
Climate Change 1995, the IPCC Second Assessment Report (SAR), was finished in 1996. It is split into four parts:
- A synthesis to help interpret UNFCCC article 2.
- The Science of Climate Change (WG I)
- Impacts, Adaptations and Mitigation of Climate Change (WG II)
- Economic and Social Dimensions of Climate Change (WG III)
Each of the last three parts was completed by a separate Working
Group (WG), and each has a Summary for Policymakers (SPM) that
represents a consensus of national representatives. The SPM of the WG I
report contains headings:
- Greenhouse gas concentrations have continued to increase
- Anthropogenic aerosols tend to produce negative radiative forcings
- Climate has changed over the past century (air temperature has increased by between 0.3 and 0.6 °C since the late 19th century; this estimate has not significantly changed since the 1990 report).
- The balance of evidence suggests a discernible human influence on global climate (considerable progress since the 1990 report in distinguishing between natural and anthropogenic influences on climate, because of: including aerosols; coupled models; pattern-based studies)
- Climate is expected to continue to change in the future (increasing realism of simulations increases confidence; important uncertainties remain but are taken into account in the range of model projections)
- There are still many uncertainties (estimates of future emissions and biogeochemical cycling; models; instrument data for model testing, assessment of variability, and detection studies)
Third assessment report
The Third Assessment Report (TAR) was completed in 2001 and consists of four reports, three of them from its Working Groups:
- Working Group I: The Scientific Basis
- Working Group II: Impacts, Adaptation and Vulnerability
- Working Group III: Mitigation
- Synthesis Report
A number of the TAR's conclusions are given quantitative estimates of
how probable it is that they are correct, e.g., greater than 66%
probability of being correct. These are "Bayesian" probabilities, which are based on an expert assessment of all the available evidence.
"Robust findings" of the TAR Synthesis Report include:
- "Observations show Earth's surface is warming. Globally, 1990s very likely warmest decade in instrumental record". Atmospheric concentrations of anthropogenic (i.e., human-emitted) greenhouse gases have increased substantially.
- Since the mid-20th century, most of the observed warming is "likely" (greater than 66% probability, based on expert judgement) due to human activities.
- Projections based on the Special Report on Emissions Scenarios suggest warming over the 21st century at a more rapid rate than that experienced for at least the last 10,000 years.
- "Projected climate change will have beneficial and adverse effects on both environmental and socio-economic systems, but the larger the changes and the rate of change in climate, the more the adverse effects predominate."
- "Ecosystems and species are vulnerable to climate change and other stresses (as illustrated by observed impacts of recent regional temperature changes) and some will be irreversibly damaged or lost."
- "Greenhouse gas emission reduction (mitigation) actions would lessen the pressures on natural and human systems from climate change."
- "Adaptation [to the effects of climate change] has the potential to reduce adverse effects of climate change and can often produce immediate ancillary benefits, but will not prevent all damages." An example of adaptation to climate change is building levees in response to sea level rise.
Comments on the TAR
In 2001, 16 national science academies issued a joint statement on climate change.
The joint statement was made by the Australian Academy of Science, the Royal Flemish Academy of Belgium for Science and the Arts, the Brazilian Academy of Sciences, the Royal Society of Canada, the Caribbean Academy of Sciences, the Chinese Academy of Sciences, the French Academy of Sciences, the German Academy of Natural Scientists Leopoldina, the Indian National Science Academy, the Indonesian Academy of Sciences, the Royal Irish Academy, Accademia Nazionale dei Lincei (Italy), the Academy of Sciences Malaysia, the Academy Council of the Royal Society of New Zealand, the Royal Swedish Academy of Sciences, and the Royal Society (UK).
The statement, also published as an editorial in the journal Science,
stated "we support the [TAR's] conclusion that it is at least 90%
certain that temperatures will continue to rise, with average global
surface temperature projected to increase by between 1.4 and 5.8 °C
above 1990 levels by 2100".
The TAR has also been endorsed by the Canadian Foundation for Climate and Atmospheric Sciences, Canadian Meteorological and Oceanographic Society, and European Geosciences Union (refer to "Endorsements of the IPCC").
In 2001, the US National Research Council (US NRC) produced a report that assessed Working Group I's (WGI) contribution to the TAR. US NRC (2001)
"generally agrees" with the WGI assessment, and describes the full WGI
report as an "admirable summary of research activities in climate
science".
IPCC author Richard Lindzen has made a number of criticisms of the TAR.
Among his criticisms, Lindzen has stated that the WGI Summary for
Policymakers (SPM) does not faithfully summarize the full WGI report. For example, Lindzen states that the SPM understates the uncertainty associated with climate models. John Houghton, who was a co-chair of TAR WGI, has responded to Lindzen's criticisms of the SPM.
Houghton has stressed that the SPM is agreed upon by delegates from
many of the world's governments, and that any changes to the SPM must be
supported by scientific evidence.
IPCC author Kevin Trenberth has also commented on the WGI SPM.
Trenberth has stated that during the drafting of the WGI SPM, some
government delegations attempted to "blunt, and perhaps obfuscate, the
messages in the report". However, Trenberth concludes that the SPM is a "reasonably balanced summary".
US NRC (2001) concluded that the WGI SPM and Technical Summary are "consistent" with the full WGI report. US NRC (2001) stated:
[...] the full [WGI] report is adequately summarized in the Technical Summary. The full WGI report and its Technical Summary are not specifically directed at policy. The Summary for Policymakers reflects less emphasis on communicating the basis for uncertainty and a stronger emphasis on areas of major concern associated with human-induced climate change. This change in emphasis appears to be the result of a summary process in which scientists work with policy makers on the document. Written responses from U.S. coordinating and lead scientific authors to the committee indicate, however, that (a) no changes were made without the consent of the convening lead authors (this group represents a fraction of the lead and contributing authors) and (b) most changes that did occur lacked significant impact.
Fourth assessment report
The Fourth Assessment Report (AR4) was published in 2007. Like previous assessment reports, it consists of four reports:
- Working Group I: The Physical Science Basis
- Working Group II: Impacts, Adaptation and Vulnerability
- Working Group III: Mitigation
- Synthesis Report
People from over 130 countries contributed to the IPCC Fourth Assessment Report, which took 6 years to produce.
Contributors to AR4 included more than 2500 scientific expert
reviewers, more than 800 contributing authors, and more than 450 lead
authors.
"Robust findings" of the Synthesis report include:
- "Warming of the climate system is unequivocal, as is now evident from observations of increases in global average air and ocean temperatures, widespread melting of snow and ice and rising global average sea level".
- Most of the global average warming over the past 50 years is "very likely" (greater than 90% probability, based on expert judgement) due to human activities.
- "Impacts [of climate change] will very likely increase due to increased frequencies and intensities of some extreme weather events".
- "Anthropogenic warming and sea level rise would continue for centuries even if GHG emissions were to be reduced sufficiently for GHG concentrations to stabilise, due to the time scales associated with climate processes and feedbacks". Stabilization of atmospheric greenhouse gas concentrations is discussed in climate change mitigation.
- "Some planned adaptation (of human activities) is occurring now; more extensive adaptation is required to reduce vulnerability to climate change".
- "Unmitigated climate change would, in the long term, be likely to exceed the capacity of natural, managed and human systems to adapt".
- "Many impacts [of climate change] can be reduced, delayed or avoided by mitigation".
Global warming projections from AR4
are shown below. The projections apply to the end of the 21st century
(2090–99), relative to temperatures at the end of the 20th century
(1980–99). Add 0.7 °C to projections to make them relative to
pre-industrial levels instead of 1980–99. (UK Royal Society, 2010, p=10. Descriptions of the greenhouse gas emissions scenarios can be found in Special Report on Emissions Scenarios.
| Emissions scenario |
Best estimate (°C) |
"Likely" range (°C) |
|---|---|---|
| B1 | 1.8 | 1.1 – 2.9 |
| A1T | 2.4 | 1.4 – 3.8 |
| B2 | 2.4 | 1.4 – 3.8 |
| A1B | 2.8 | 1.7 – 4.4 |
| A2 | 3.4 | 2.0 – 5.4 |
| A1FI | 4.0 | 2.4 – 6.4 |
"Likely" means greater than 66% probability of being correct, based on expert judgement.
Response to AR4
Several science academies have referred to and/or reiterated some of the conclusions of AR4. These include:
- Joint-statements made in 2007, 2008, and 2009 by the science academies of Brazil, China, India, Mexico, South Africa and the G8 nations (the "G8+5").
- Publications by the Australian Academy of Science.
- A joint-statement made in 2007 by the Network of African Science Academies.
- A statement made in 2010 by the Inter Academy Medical Panel This statement has been signed by 43 scientific academies.
The Netherlands Environmental Assessment Agency (PBL, et al., 2009; 2010) has carried out two reviews of AR4. These reviews are generally supportive of AR4's conclusions. PBL (2010)
make some recommendations to improve the IPCC process. A literature
assessment by the US National Research Council (US NRC, 2010) concludes:
Climate change is occurring, is caused largely by human activities, and poses significant risks for—and in many cases is already affecting—a broad range of human and natural systems [emphasis in original text]. [...] This conclusion is based on a substantial array of scientific evidence, including recent work, and is consistent with the conclusions of recent assessments by the U.S. Global Change Research Program [...], the Intergovernmental Panel on Climate Change’s Fourth Assessment Report [...], and other assessments of the state of scientific knowledge on climate change.
Some errors have been found in the IPCC AR4 Working Group II report. Two errors include the melting of Himalayan glaciers, and Dutch land area that is below sea level.
Fifth assessment report
The IPCC's Fifth Assessment Report (AR5) was completed in 2014. AR5 followed the same general format as of AR4, with three Working Group reports and a Synthesis report. The Working Group I report (WG1) was published in September 2013.
Conclusions of AR5 are summarized below:
- Working Group I
- "Warming of the climate system is unequivocal, and since the 1950s, many of the observed changes are unprecedented over decades to millennia".
- "Atmospheric concentrations of carbon dioxide, methane, and nitrous oxide have increased to levels unprecedented in at least the last 800,000 years".
- Human influence on the climate system is clear. It is extremely likely (95-100% probability) that human influence was the dominant cause of global warming between 1951-2010.
- Working Group II
- "Increasing magnitudes of [global] warming increase the likelihood of severe, pervasive, and irreversible impacts"
- "A first step towards adaptation to future climate change is reducing vulnerability and exposure to present climate variability"
- "The overall risks of climate change impacts can be reduced by limiting the rate and magnitude of climate change"
- Working Group III
- Without new policies to mitigate climate change, projections suggest an increase in global mean temperature in 2100 of 3.7 to 4.8 °C, relative to pre-industrial levels (median values; the range is 2.5 to 7.8 °C including climate uncertainty).
- The current trajectory of global greenhouse gas emissions is not consistent with limiting global warming to below 1.5 or 2 °C, relative to pre-industrial levels. Pledges made as part of the Cancún Agreements are broadly consistent with cost-effective scenarios that give a "likely" chance (66-100% probability) of limiting global warming (in 2100) to below 3 °C, relative to pre-industrial levels.
Representative Concentration Pathways
Projections in AR5 are based on "Representative Concentration Pathways" (RCPs).[86]
The RCPs are consistent with a wide range of possible changes in future
anthropogenic greenhouse gas emissions. Projected changes in global
mean surface temperature and sea level are given in the main RCP article.
Special reports
In
addition to climate assessment reports, the IPCC publishes Special
Reports on specific topics. The preparation and approval process for all
IPCC Special Reports follows the same procedures as for IPCC Assessment
Reports. In the year 2011 two IPCC Special Report were finalized, the
Special Report on Renewable Energy Sources and Climate Change Mitigation
(SRREN) and the Special Report on Managing Risks of Extreme Events and
Disasters to Advance Climate Change Adaptation (SREX). Both Special
Reports were requested by governments.
Special Report on Emissions Scenarios (SRES)
The Special Report on Emissions Scenarios (SRES) is a report by the IPCC which was published in 2000. The SRES contains "scenarios" of future changes in emissions of greenhouse gases and sulfur dioxide.
One of the uses of the SRES scenarios is to project future changes in
climate, e.g., changes in global mean temperature. The SRES scenarios
were used in the IPCC's Third and Fourth Assessment Reports.
The SRES scenarios are "baseline" (or "reference") scenarios,
which means that they do not take into account any current or future
measures to limit greenhouse gas (GHG) emissions (e.g., the Kyoto Protocol to the United Nations Framework Convention on Climate Change).
SRES emissions projections are broadly comparable in range to the
baseline projections that have been developed by the scientific
community.
Comments on the SRES
There have been a number of comments on the SRES. Parson et al. (2007)
stated that the SRES represented "a substantial advance from prior
scenarios". At the same time, there have been criticisms of the SRES.
The most prominently publicized criticism of SRES focused on the
fact that all but one of the participating models compared gross
domestic product (GDP) across regions using market exchange rates (MER), instead of the more correct purchasing-power parity (PPP) approach. This criticism is discussed in the main SRES article.
Special report on renewable energy sources and climate change mitigation (SRREN)
This report assesses existing literature on renewable energy commercialisation
for the mitigation of climate change. It was published in 2012 and
covers the six most important renewable energy technologies, as well as
their integration into present and future energy systems. It also takes
into consideration the environmental and social consequences associated
with these technologies, the cost and strategies to overcome technical
as well as non-technical obstacles to their application and diffusion.
The full report in PDF form is found here.
More than 130 authors from all over the world contributed to the
preparation of IPCC Special Report on Renewable Energy Sources and
Climate Change Mitigation (SRREN) on a voluntary basis – not to mention
more than 100 scientists, who served as contributing authors.
Special Report on managing the risks of extreme events and disasters to advance climate change adaptation (SREX)
The report
was published in 2012. It assesses the effect that climate change has
on the threat of natural disasters and how nations can better manage an
expected change in the frequency of occurrence and intensity of severe
weather patterns. It aims to become a resource for decision-makers to
prepare more effectively for managing the risks of these events. A
potentially important area for consideration is also the detection of
trends in extreme events and the attribution of these trends to human
influence. The full report, 594 pages in length, may be found here in PDF form.
More than 80 authors, 19 review editors, and more than 100
contributing authors from all over the world contributed to the
preparation of SREX.
Special Report on Global Warming of 1.5 °C (SR15)
When the Paris Agreement was adopted, the UNFCCC
invited the Intergovernmental Panel on Climate Change to write a
special report on "How can humanity prevent the global temperature rise
more than 1.5 degrees above pre-industrial level". The completed report, Special Report on Global Warming of 1.5 °C
(SR15), was released on October 8, 2018. Its full title is "Global
Warming of 1.5 °C, an IPCC special report on the impacts of global
warming of 1.5 °C above pre-industrial levels and related global
greenhouse gas emission pathways, in the context of strengthening the
global response to the threat of climate change, sustainable
development, and efforts to eradicate poverty".
The finished report summarizes the findings of scientists,
showing that maintaining a temperature rise to below 1.5 °C remains
possible, but only through "rapid and far-reaching transitions in
energy, land, urban and infrastructure..., and industrial systems". Meeting the Paris target of 1.5 °C (2.7 °F) is possible but would require "deep emissions reductions", "rapid", "far-reaching and unprecedented changes in all aspects of society".
In order to achieve the 1.5 °C target, CO2 emissions must decline by
45% (relative to 2010 levels) by 2030, reaching net zero by around 2050.
Deep reductions in non-CO2 emissions (such as nitrous oxide and
methane) will also be required to limit warming to 1.5 °C. Under the
pledges of the countries entering the Paris Accord, a sharp rise of 3.1
to 3.7 °C is still expected to occur by 2100. Holding this rise to
1.5 °C avoids the worst effects of a rise by even 2 °C. However, a
warming of even 1.5 degrees will still result in large-scale drought,
famine, heat stress, species die-off, loss of entire ecosystems, and
loss of habitable land, throwing more than 100 Million into poverty.
Effects will be most drastic in arid regions including the Middle East and the Sahel
in Africa, where fresh water will remain in some areas following a
1.5 °C rise in temperatures but are expected to dry up completely if the
rise reaches 2 °C.
Special Report on climate change and land (SRCCL)
The final draft of the "Special Report on climate change and land"
(SRCCL)—with the full title, "Special Report on climate change,
desertification, land degradation, sustainable land management, food
security, and greenhouse gas fluxes in terrestrial ecosystems" was
published online on August 7, 2019.
The SRCCL consists of seven chapters, Chapter 1: Framing and Context,
Chapter 2: Land-Climate Interactions, Chapter 3: Desertification,
Chapter 4: Land Degradation, Chapter 5: Food Security, Chapter 5
Supplementary Material, Chapter 6: Interlinkages between
desertification, land degradation, food security and GHG fluxes:
Synergies, trade-offs and Integrated Response Options, and Chapter 7:
Risk management and decision making in relation to sustainable
development.
Special Report on the Ocean and Cryosphere in a Changing Climate (SROCC)
The "Special Report on the Ocean and Cryosphere in a Changing Climate" (SROCC) was approved on September 25, 2019 in Monaco.
Among other findings, the report concluded that sea level rises could
be up to two feet higher by the year 2100, even if efforts to reduce
greenhouse gas emissions and to limit global warming are successful;
coastal cities across the world could see so-called "storm[s] of the
century" at least once a year.
Methodology reports
Within IPCC the National Greenhouse Gas Inventory Program develops methodologies to estimate emissions of greenhouse gases. This has been undertaken since 1991 by the IPCC WGI in close collaboration with the Organisation for Economic Co-operation and Development and the International Energy Agency.
The objectives of the National Greenhouse Gas Inventory Program are:
- to develop and refine an internationally agreed methodology and software for the calculation and reporting of national greenhouse gas emissions and removals; and
- to encourage the widespread use of this methodology by countries participating in the IPCC and by signatories of the UNFCCC.
Revised 1996 IPCC Guidelines for National Greenhouse Gas Inventories
The
1996 Guidelines for National Greenhouse Gas Investories provide the
methodological basis for the estimation of national greenhouse gas emissions inventories. Over time these guidelines have been completed with good practice reports: Good Practice Guidance and Uncertainty Management in National Greenhouse Gas Inventories and Good Practice Guidance for Land Use, Land-Use Change and Forestry.
The 1996 guidelines and the two good practice reports are to be used by parties to the UNFCCC and to the Kyoto Protocol in their annual submissions of national greenhouse gas inventories.
2006 IPCC Guidelines for National Greenhouse Gas Inventories
The 2006 IPCC Guidelines for National Greenhouse Gas Inventories is the latest version of these emission estimation methodologies, including a large number of default emission factors.
Although the IPCC prepared this new version of the guidelines on
request of the parties to the UNFCCC, the methods have not yet been
officially accepted for use in national greenhouse gas emissions
reporting under the UNFCCC and the Kyoto Protocol.
Activities
The
IPCC concentrates its activities on the tasks allotted to it by the
relevant WMO Executive Council and UNEP Governing Council resolutions
and decisions as well as on actions in support of the UNFCCC process.
While the preparation of the assessment reports is a major IPCC
function, it also supports other activities, such as the Data
Distribution Centre and the National Greenhouse Gas Inventories Programme, required under the UNFCCC. This involves publishing default emission factors, which are factors used to derive emissions estimates based on the levels of fuel consumption, industrial production and so on.
The IPCC also often answers inquiries from the UNFCCC Subsidiary Body for Scientific and Technological Advice (SBSTA).
Nobel Peace Prize
In December 2007, the IPCC was awarded the Nobel Peace Prize
"for their efforts to build up and disseminate greater knowledge about
man-made climate change, and to lay the foundations for the measures
that are needed to counteract such change". The award is shared with
Former U.S. Vice-President Al Gore for his work on climate change and the documentary An Inconvenient Truth.
Criticisms
There is widespread support for the IPCC in the scientific community, which is reflected in publications by other scientific bodies and experts. However, criticisms of the IPCC have been made.
Since 2010 the IPCC has come under yet unparalleled public and political scrutiny. The global IPCC consensus approach has been challenged internally and externally, for example, during the 2009 Climatic Research Unit email controversy ("Climategate"). It is contested by some as an information monopoly with results for both the quality and the impact of the IPCC work as such.
Projected date of melting of Himalayan glaciers
A paragraph in the 2007 Working Group II report ("Impacts, Adaptation
and Vulnerability"), chapter 10 included a projection that Himalayan
glaciers could disappear by 2035.
- Glaciers in the Himalaya are receding faster than in any other part of the world (see Table 10.9) and, if the present rate continues, the likelihood of them disappearing by the year 2035 and perhaps sooner is very high if the Earth keeps warming at the current rate. Its total area will likely shrink from the present 500,000 to 100,000 km2 by the year 2035 (WWF, 2005).
This projection was not included in the final summary for
policymakers. The IPCC has since acknowledged that the date is
incorrect, while reaffirming that the conclusion in the final summary
was robust. They expressed regret for "the poor application of
well-established IPCC procedures in this instance". The date of 2035 has
been correctly quoted by the IPCC from the WWF report, which has
misquoted its own source, an ICSI report "Variations of Snow and Ice in the past and at present on a Global and Regional Scale"
.
Rajendra K. Pachauri responded in an interview with Science.
Overstatement of effects
Former IPCC chairman Robert Watson
said, regarding the Himalayan glaciers estimation, "The mistakes all
appear to have gone in the direction of making it seem like climate
change is more serious by overstating the impact. That is worrying. The
IPCC needs to look at this trend in the errors and ask why it happened". Martin Parry, a climate expert
who had been co-chair of the IPCC working group II, said that "What
began with a single unfortunate error over Himalayan glaciers has become
a clamour without substance" and the IPCC had investigated the other
alleged mistakes, which were "generally unfounded and also marginal to
the assessment".
Emphasis of the "hockey stick" graph

IPCC WG1 Co-chair Sir John T. Houghton showing the IPCC fig. 2.20 hockey stick graph at a climate conference in 2005
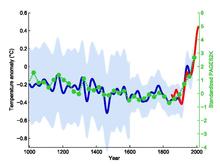
The original northern hemisphere hockey stick graph of Mann, Bradley & Hughes 1999,
smoothed curve shown in blue with its uncertainty range in light blue,
overlaid with green dots showing the 30-year global average of the PAGES 2k Consortium 2013 reconstruction. The red curve shows measured global mean temperature, according to HadCRUT4 data from 1850 to 2013.

Figure 3.20 on p.175 of the IPCC Second Assessment Report.

Comparison of MBH99 40-year average from proxy records, as used in IPCC TAR 2001 (blue), with IPCC 1990
schematic Figure 7.1.c (red) [based on Lamb 1965 extrapolating from
central England temperatures and other historical records]; central
England temperatures to 2007 shown from Jones et al. 2009 (green dashed line). Also shown, Moberg et al. 2005 low frequency signal (black).
The third assessment report (TAR) prominently featured a graph labeled "Millennial Northern Hemisphere temperature reconstruction" based on a 1999 paper by Michael E. Mann, Raymond S. Bradley and Malcolm K. Hughes (MBH99), which has been referred to as the "hockey stick graph". This graph extended the similar graph in Figure 3.20 from the IPCC Second Assessment Report of 1995, and differed from a schematic in the first assessment report
that lacked temperature units, but appeared to depict larger global
temperature variations over the past 1000 years, and higher temperatures
during the Medieval Warm Period
than the mid 20th century. The schematic was not an actual plot of
data, and was based on a diagram of temperatures in central England,
with temperatures increased on the basis of documentary evidence of
Medieval vineyards in England.
Even with this increase, the maximum it showed for the Medieval Warm
Period did not reach temperatures recorded in central England in 2007. The MBH99 finding was supported by cited reconstructions by Jones et al. 1998, Pollack, Huang & Shen 1998, Crowley & Lowery 2000 and Briffa 2000,
using differing data and methods. The Jones et al. and Briffa
reconstructions were overlaid with the MBH99 reconstruction in Figure
2.21 of the IPCC report.
These studies were widely presented as demonstrating that the
current warming period is exceptional in comparison to temperatures
between 1000 and 1900, and the MBH99 based graph featured in publicity.
Even at the draft stage, this finding was disputed by contrarians: in
May 2000 Fred Singer's Science and Environmental Policy Project held a press event on Capitol Hill, Washington, D.C., featuring comments on the graph Wibjörn Karlén and Singer argued against the graph at a United States Senate Committee on Commerce, Science and Transportation hearing on 18 July 2000. Contrarian John Lawrence Daly
featured a modified version of the IPCC 1990 schematic, which he
mis-identified as appearing in the IPCC 1995 report, and argued that
"Overturning its own previous view in the 1995 report, the IPCC
presented the 'Hockey Stick' as the new orthodoxy with hardly an apology
or explanation for the abrupt U-turn since its 1995 report". Criticism of the MBH99 reconstruction in a review paper, which was quickly discredited in the Soon and Baliunas controversy, was picked up by the Bush administration, and a Senate speech by US Republican senator James Inhofe
alleged that "manmade global warming is the greatest hoax ever
perpetrated on the American people". The data and methodology used to
produce the "hockey stick graph" was criticized in papers by Stephen McIntyre and Ross McKitrick, and in turn the criticisms in these papers were examined by other studies and comprehensively refuted by Wahl & Ammann 2007, which showed errors in the methods used by McIntyre and McKitrick.
On 23 June 2005, Rep. Joe Barton, chairman of the House Committee on Energy and Commerce wrote joint letters with Ed Whitfield, chairman of the Subcommittee on Oversight and Investigations
demanding full records on climate research, as well as personal
information about their finances and careers, from Mann, Bradley and
Hughes. Sherwood Boehlert, chairman of the House Science Committee,
said this was a "misguided and illegitimate investigation" apparently
aimed at intimidating scientists, and at his request the U.S. National Academy of Sciences arranged for its National Research Council to set up a special investigation.
The National Research Council's report agreed that there were some
statistical failings, but these had little effect on the graph, which
was generally correct. In a 2006 letter to Nature,
Mann, Bradley, and Hughes pointed out that their original article had
said that "more widespread high-resolution data are needed before more
confident conclusions can be reached" and that the uncertainties were
"the point of the article".
The IPCC Fourth Assessment Report
(AR4) published in 2007 featured a graph showing 12 proxy based
temperature reconstructions, including the three highlighted in the 2001
Third Assessment Report (TAR); Mann, Bradley & Hughes 1999 as before, Jones et al. 1998 and Briffa 2000 had both been calibrated by newer studies. In addition, analysis of the Medieval Warm Period cited reconstructions by Crowley & Lowery 2000 (as cited in the TAR) and Osborn & Briffa 2006.
Ten of these 14 reconstructions covered 1,000 years or longer. Most
reconstructions shared some data series, particularly tree ring data,
but newer reconstructions used additional data and covered a wider area,
using a variety of statistical methods. The section discussed the divergence problem affecting certain tree ring data.
Conservative nature of IPCC reports
Some critics have contended that the IPCC reports tend to be conservative by consistently underestimating the pace and impacts of global warming, and report only the "lowest common denominator" findings.
On the eve of the publication of IPCC's Fourth Assessment Report
in 2007 another study was published suggesting that temperatures and
sea levels have been rising at or above the maximum rates proposed
during IPCC's 2001 Third Assessment Report.
The study compared IPCC 2001 projections on temperature and sea level
change with observations. Over the six years studied, the actual
temperature rise was near the top end of the range given by IPCC's 2001
projection, and the actual sea level rise was above the top of the range
of the IPCC projection.
Another example of scientific research which suggests that
previous estimates by the IPCC, far from overstating dangers and risks,
have actually understated them is a study on projected rises in sea
levels. When the researchers' analysis was "applied to the possible
scenarios outlined by the Intergovernmental Panel on Climate Change
(IPCC), the researchers found that in 2100 sea levels would be 0.5–1.4 m
[50–140 cm] above 1990 levels. These values are much greater than the
9–88 cm as projected by the IPCC itself in its Third Assessment Report,
published in 2001". This may have been due, in part, to the expanding
human understanding of climate.
Greg Holland from the National Center for Atmospheric Research, who reviewed a multi-meter sea level rise study by Jim Hansen, noted “There
is no doubt that the sea level rise, within the IPCC, is a very
conservative number, so the truth lies somewhere between IPCC and Jim.”
In reporting criticism by some scientists that IPCC's
then-impending January 2007 report understates certain risks,
particularly sea level rises, an AP story quoted Stefan Rahmstorf,
professor of physics and oceanography at Potsdam University as saying
"In a way, it is one of the strengths of the IPCC to be very
conservative and cautious and not overstate any climate change risk".
In his December 2006 book, Hell and High Water: Global Warming, and in an interview on Fox News on 31 January 2007, energy expert Joseph Romm noted that the IPCC Fourth Assessment Report
is already out of date and omits recent observations and factors
contributing to global warming, such as the release of greenhouse gases
from thawing tundra.
Political influence on the IPCC has been documented by the
release of a memo by ExxonMobil to the Bush administration, and its
effects on the IPCC's leadership. The memo led to strong Bush
administration lobbying, evidently at the behest of ExxonMobil, to oust Robert Watson,
a climate scientist, from the IPCC chairmanship, and to have him
replaced by Pachauri, who was seen at the time as more mild-mannered and
industry-friendly.
IPCC processes
Michael Oppenheimer, a long-time participant in the IPCC and coordinating lead author of the Fifth Assessment Report conceded in Science Magazine's State of the Planet 2008–2009
some limitations of the IPCC consensus approach and asks for
concurring, smaller assessments of special problems instead of the large
scale approach as in the previous IPCC assessment reports. It has become more important to provide a broader exploration of uncertainties.
Others see as well mixed blessings of the drive for consensus within
the IPCC process and ask to include dissenting or minority positions or to improve statements about uncertainties.
The IPCC process on climate change and its efficiency and success
has been compared with dealings with other environmental challenges. In case of the Ozone depletion, global regulation based on the Montreal Protocol has been successful. In case of Climate Change, the Kyoto Protocol failed. The Ozone case was used to assess the efficiency of the IPCC process.
The lockstep situation of the IPCC is having built a broad science
consensus while states and governments still follow different, if not
opposing goals. The underlying linear model of policy-making of the more knowledge we have, the better the political response will be is being doubted.
According to Sheldon Ungar's comparison with global warming, the
actors in the ozone depletion case had a better understanding of
scientific ignorance and uncertainties. The ozone case communicated to lay persons "with easy-to-understand bridging metaphors derived from the popular culture" and related to "immediate risks with everyday relevance", while the public opinion on climate change sees no imminent danger.
The stepwise mitigation of the ozone layer challenge was based as well
on successfully reducing regional burden sharing conflicts.
In case of the IPCC conclusions and the failure of the Kyoto Protocol,
varying regional cost-benefit analysis and burden-sharing conflicts with
regard to the distribution of emission reductions remain an unsolved
problem.
In the UK, a report for a House of Lords committee asked to urge the
IPCC to involve better assessments of costs and benefits of climate
change, but the Stern Review, ordered by the UK government, made a stronger argument in favor to combat human-made climate change.
Outdatedness of reports
Since
the IPCC does not carry out its own research, it operates on the basis
of scientific papers and independently documented results from other
scientific bodies, and its schedule for producing reports requires a
deadline for submissions prior to the report's final release. In
principle, this means that any significant new evidence or events that
change our understanding of climate science between this deadline and
publication of an IPCC report cannot be included. In an area of science
where our scientific understanding is rapidly changing, this has been
raised as a serious shortcoming in a body which is widely regarded as
the ultimate authority on the science. However, there has generally been a steady evolution of key findings and levels of scientific confidence from one assessment report to the next.
The submission deadlines for the Fourth Assessment Report (AR4)
differed for the reports of each Working Group. Deadlines for the
Working Group I report were adjusted during the drafting and review
process in order to ensure that reviewers had access to unpublished
material being cited by the authors. The final deadline for cited
publications was 24 July 2006. The final WG I report was released on 30 April 2007 and the final AR4 Synthesis Report was released on 17 November 2007.Rajendra Pachauri,
the IPCC chair, admitted at the launch of this report that since the
IPCC began work on it, scientists have recorded "much stronger trends in
climate change", like the unforeseen dramatic melting of polar ice in
the summer of 2007, and added, "that means you better start with intervention much earlier".
Burden on participating scientists
Scientists
who participate in the IPCC assessment process do so without any
compensation other than the normal salaries they receive from their home
institutions. The process is labor-intensive, diverting time and
resources from participating scientists' research programs.
Concerns have been raised that the large uncompensated time commitment
and disruption to their own research may discourage qualified scientists
from participating.
Lack of error correction after publication
In
May 2010, Pachauri noted that the IPCC currently had no process for
responding to errors or flaws once it issued a report. The problem,
according to Pachauri, was that once a report was issued the panels of
scientists producing the reports were disbanded.
Proposed organizational overhaul
In February 2010, in response to controversies regarding claims in the Fourth Assessment Report, five climate scientists – all contributing or lead IPCC report authors – wrote in the journal Nature
calling for changes to the IPCC. They suggested a range of new
organizational options, from tightening the selection of lead authors
and contributors, to dumping it in favor of a small permanent body, or
even turning the whole climate science assessment process into a moderated "living" Wikipedia-IPCC.
Other recommendations included that the panel employ a full-time staff
and remove government oversight from its processes to avoid political
interference.
Reframing of scientific research
The 2018 report What Lies Beneath by the Breakthrough - National Centre for Climate Restoration, with contributions from Kevin Anderson, James Hansen, Michael E. Mann, Michael Oppenheimer, Naomi Oreskes, Stefan Rahmstorf, Eric Rignot, Hans Joachim Schellnhuber, Kevin Trenberth,
and others, urges the IPCC, the wider UNFCCC negotiations, and national
policy makers to change their approach. The authors note, "We urgently
require a reframing of scientific research within an existential
risk-management framework."
InterAcademy Council review
In March 2010, at the invitation of the United Nations secretary-general and the chair of the IPCC, the InterAcademy Council (IAC) was asked to review the IPCC's processes for developing its reports. The IAC panel, chaired by Harold Tafler Shapiro, convened on 14 May 2010 and released its report on 1 September 2010.
The IAC found that, "The IPCC assessment process has been
successful overall". The panel, however, made seven formal
recommendations for improving the IPCC's assessment process, including:
- establish an executive committee;
- elect an executive director whose term would only last for one assessment;
- encourage review editors to ensure that all reviewer comments are adequately considered and genuine controversies are adequately reflected in the assessment reports;
- adopt a better process for responding to reviewer comments;
- working groups should use a qualitative level-of-understanding scale in the Summary for Policy Makers and Technical Summary;
- "Quantitative probabilities (as in the likelihood scale) should be used to describe the probability of well-defined outcomes only when there is sufficient evidence"; and
- implement a communications plan that emphasizes transparency and establish guidelines for who can speak on behalf of the organization.
The panel also advised that the IPCC avoid appearing to advocate specific policies in response to its scientific conclusions. Commenting on the IAC report, Nature News
noted that "The proposals were met with a largely favourable response
from climate researchers who are eager to move on after the media
scandals and credibility challenges that have rocked the United Nations
body during the past nine months".
Archiving
Papers
and electronic files of certain working groups of the IPCC, including
reviews and comments on drafts of their Assessment Reports, are archived
at the Environmental Science and Public Policy Archives in the Harvard Library.
Endorsements of the IPCC
Various scientific bodies have issued official statements endorsing and concurring with the findings of the IPCC.
- Joint science academies' statement of 2001. "The work of the Intergovernmental Panel on Climate Change (IPCC) represents the consensus of the international scientific community on climate change science. We recognise IPCC as the world's most reliable source of information on climate change and its causes, and we endorse its method of achieving this consensus".
- Canadian Foundation for Climate and Atmospheric Sciences. "We concur with the climate science assessment of the Intergovernmental Panel on Climate Change (IPCC) in 2001 ... We endorse the conclusions of the IPCC assessment..."
- Canadian Meteorological and Oceanographic Society. "CMOS endorses the process of periodic climate science assessment carried out by the Intergovernmental Panel on Climate Change and supports the conclusion, in its Third Assessment Report, which states that the balance of evidence suggests a discernible human influence on global climate."
- European Geosciences Union. "The Intergovernmental Panel on Climate Change [...] is the main representative of the global scientific community [...][The] IPCC third assessment report [...] represents the state-of-the-art of climate science supported by the major science academies around the world and by the vast majority of scientific researchers and investigations as documented by the peer-reviewed scientific literature".
- International Council for Science (ICSU). "...the IPCC 4th Assessment Report represents the most comprehensive international scientific assessment ever conducted. This assessment reflects the current collective knowledge on the climate system, its evolution to date, and its anticipated future development".
- National Oceanic and Atmospheric Administration (USA). "Internationally, the Intergovernmental Panel on Climate Change (IPCC)... is the most senior and authoritative body providing scientific advice to global policy makers".
- United States National Research Council. "The IPCC Third Assessment Report'] conclusion that most of the observed warming of the last 50 years is likely to have been due to the increase in greenhouse gas concentrations accurately reflects the current thinking of the scientific community on this issue".
- Network of African Science Academies. "The IPCC should be congratulated for the contribution it has made to public understanding of the nexus that exists between energy, climate and sustainability".
- Royal Meteorological Society, in response to the release of the Fourth Assessment Report, referred to the IPCC as "The world's best climate scientists".
- Stratigraphy Commission of the Geological Society of London. "The most authoritative assessment of climate change in the near future is provided by the Inter-Governmental Panel for Climate Change".


_(8249451687).jpg)



